Shoulder impingement occurs when the rotator cuff tendons become pinched beneath the acromion. That repeated compression creates friction during arm movement and gradually causes tendon swelling and fraying.
Early recognition prevents a mild irritation from progressing into a partial or full tendon tear. Many people ignore the symptoms until night pain interrupts sleep or simple lifting tasks become difficult.
The first sign is usually a dull ache during overhead reaching rather than sudden sharp pain. The second sign is unexplained weakness, such as difficulty lifting a coffee cup or reaching into a cabinet. Let's look at shoulder impingement symptoms and how to recognize them early.
What Is Shoulder Impingement?
The shoulder joint relies on a narrow passage called the subacromial space. Tendons of the rotator cuff and the bursa pass through this space beneath the acromion bone.

Impingement occurs when that space narrows enough to compress the tendons with each arm raise. Repetitive compression leads to tendon inflammation and progressive fraying without a sudden injury.
- The Role of the Acromion
The acromion forms the roof of the shoulder. Its shape varies from flat to curved to hooked.
A hooked acromion reduces the subacromial space more than a flat one. That shape difference explains why some people develop impingement earlier than others.
- The Pinch During Arm Lifts
Each time you lift your arm above shoulder height, the greater tuberosity of the humerus moves under the acromion. The rotator cuff tendons sit directly between these two bones.
Normal elevation creates a small amount of tendon compression. In impingement, that compression crosses the line into mechanical irritation and tissue damage.
- Why the Bursa Matters
The subacromial bursa acts as a cushion between tendon and bone. Chronic compression irritates the bursa first.
An irritated bursa swells and takes up more space inside an already tight area. That swelling makes the impingement worse by further narrowing the passage for the tendons.
First Signs You Should Not Ignore
Pain that starts as a mild ache in the front or side of the shoulder rarely feels urgent. That ache often appears after repetitive overhead activity like painting or swimming.
Weakness without a clear injury marks an early red flag. You might notice trouble lifting a small object or a sense that the arm gives out during simple tasks.
- Pain During Overhead Reach
Lifting the arm to shoulder height or above triggers a distinct pinch. The pain typically sits on the top or front of the shoulder, not deep inside the joint.
Reaching forward feels easier than reaching sideways. This difference occurs because sideways lifting narrows the subacromial space more than forward lifting.
- Night Pain on the Affected Side
Lying on the impinged shoulder compresses the already inflamed tendons. Many people wake up when they roll onto that side during sleep.
Pain also appears when lifting the arm while lying flat on the back. Gravity pulls the humeral head upward into the acromion in that position.
- Loss of Full Range
Reaching behind the back to tuck in a shirt becomes difficult. Reaching behind to fasten a zipper or hook a bra also causes discomfort.
The motion loss starts gradually. Complete loss of movement usually indicates another condition such as frozen shoulder.
How the Pain Changes Over Time
Early impingement produces pain only during specific arm movements. Rest and activity modification usually resolve that pain within hours.

As tendon irritation progresses, pain lingers after the movement stops. Grocery shopping in the morning might cause discomfort that lasts into the afternoon.
- From Dull Ache to Sharp Twinge
The initial sensation resembles a toothache inside the shoulder joint. That dull quality makes it easy to dismiss as muscle soreness from exercise.
Sharp pain replaces the dull ache once inflammation reaches a critical level. A sudden twinge during a routine reach, like grabbing a coffee mug, signals worsening pathology.
- Morning Stiffness Versus Daytime Pain
Morning stiffness without night pain points to early stage impingement. Tendons settle and stiffen during sleep but do not yet hurt while lying still.
Daytime pain that worsens with each hour of use indicates more advanced irritation. The cumulative effect of repeated arm lifts throughout the day produces this pattern.
- Pain That Referrals Down the Arm
Impingement pain often travels from the front of the shoulder to the outer arm. That referral stops near the elbow and does not go past it.
Pain past the elbow into the hand suggests nerve involvement. Cervical spine problems or thoracic outlet syndrome produce that different pattern.
Where You Actually Feel the Pain
The front of the shoulder near the collarbone holds the most common pain site. Patients point to the spot where the deltoid muscle meets the upper chest.
Pain localized to the top of the shoulder directly under the acromion also occurs frequently. That location corresponds to the primary compression point between bone and tendon.
| Pain Location | Likely Source | Typical Referral Pattern |
| Front of shoulder near collarbone | Supraspinatus tendon compression | Stops at the elbow |
| Top of shoulder under acromion | Subacromial bursa irritation | No referral past mid arm |
| Outer upper arm along deltoid | C5 nerve root referral from inflammation | Travels down but not to hand |
| Back of shoulder near scapula | Not typical for impingement | Suggests labral or rotator cuff tear |
| Past elbow into hand | Not impingement | Cervical spine or nerve entrapment |
- Outer Arm Without Hand Involvement
Pain spreads down the outside of the upper arm along the deltoid muscle. This referral pattern follows the dermatome of the C5 nerve root which supplies the rotator cuff.
The hand and fingers remain pain free in pure impingement. Numbness or tingling in the digits suggests a separate nerve compression syndrome.
- Deep Ache Versus Surface Tenderness
Deep pain felt inside the joint without a precise trigger point characterizes early impingement. Patients struggle to locate the exact sore spot with one finger.
Surface tenderness develops later when the bursa becomes chronically inflamed. Pressing on the lateral acromion reproduces pain at that stage.
- Pain That Avoids the Back of the Shoulder
Impingement rarely causes pain behind the shoulder near the scapula. Posterior shoulder pain points more toward rotator cuff tear or labral pathology.
Pain that centers on the top of the shoulder blade instead suggests acromioclavicular joint arthritis. That separate condition often accompanies impingement but produces a distinct pain location.
Movements That Often Trigger Symptoms
Lifting the arm sideways, a motion called abduction, creates the most consistent pain. The pinch usually starts when the arm reaches 60° to 120° away from the body.
Reaching forward to shoulder height causes less pain than lifting sideways. The shoulder mechanics change just enough to widen the subacromial space during forward flexion.
| Movement | Pain Onset Angle | Intensity Level |
| Sideways lift (abduction) | 60° to 120° | High |
| Forward lift (flexion) | 90° to 140° | Mild to moderate |
| Reaching behind back | Any angle | Moderate |
| Overhead press | 100° to 180 ° | High |
| Carrying at side | No pain with small loads | Low |
- The Painful Arc
Pain appears when the arm moves between 60° and 120° of sideways lift. That specific range narrows the subacromial space to its smallest measurement.
Pain disappears once the arm passes 120°. The greater tuberosity moves under the acromion and no longer compresses the tendons at that height.
- Reaching Behind the Body
Tucking a shirt into pants or fastening a back zipper requires internal rotation. That movement presses the supraspinatus tendon directly against the anterior acromion.
Reaching behind to wash the opposite shoulder blade produces the same compression. Patients often report switching hands for back hygiene tasks.
- Lifting With the Arm Straight
Carrying a suitcase or grocery bag at the side triggers less pain than lifting the same weight overhead. The tendons remain under the acromion but experience lower compression force.
Lifting an object with the arm extended forward at shoulder height reproduces the pinch. The lever arm effect multiplies the load on the already irritated tendons.
Weakness Without Warning
True weakness occurs without muscle atrophy in early impingement. The pain itself inhibits full muscle contraction through a reflex called arthrogenic muscle inhibition.
Lifting the arm sideways meets sudden resistance that feels like the arm gives out. This pseudo-weakness disappears when a doctor numbs the subacromial space.
- Trouble Lifting Everyday Items
A half gallon of milk or a full laundry basket becomes difficult to carry at the side. The shoulder tires faster than the unaffected side during sustained holding.
Lifting an item from a low shelf to an overhead shelf produces the most noticeable deficit. The arm shakes or gives way during the middle portion of that lift.
- Reaching Forward With Resistance
Pushing a door open or sliding a heavy pan across the stove requires shoulder stability. Impingement reduces that stability without any rotator cuff tear present.
Resisted forward elevation at waist height does not hurt as much as sideways resistance. The infraspinatus and teres minor muscles contribute more to external rotation than to forward lift.
- How Doctors Test for True Weakness
A lidocaine injection into the subacromial space temporarily removes pain. Strength that returns after the injection confirms pain inhibition rather than a tendon tear.
Strength that stays poor after anesthesia points toward a rotator cuff tear. Magnetic resonance imaging differentiates between these two causes of weakness.
How to Tell It Apart from Other Shoulder Problems
Arthritis produces deep joint pain that worsens with activity and improves with rest. Impingement pain follows the same pattern but adds the painful arc during mid range motion.
Arthritis limits all shoulder motions equally. Impingement preserves full range when the arm moves without resistance or weight.
- Frozen Shoulder Differences
Frozen shoulder causes a global loss of both active and passive motion. The patient cannot lift the arm even when a doctor moves it for them.
Impingement maintains full passive range. The doctor can lift the arm completely overhead while the patient relaxes despite the pain.
- Rotator Cuff Tear Signs
A full thickness rotator cuff tear produces weakness that persists after an anesthetic injection. The patient cannot lift the arm sideways even with the pain gone.
Impingement weakness resolves completely with that same injection. The arm lifts fully once the pain stops inhibiting the muscle.
- Cervical Spine Referral Patterns
Neck arthritis sends pain from the cervical spine down the entire arm into the hand. That pain changes with neck position more than with shoulder position.
Impingement pain stops at the elbow and does not enter the hand. Shoulder position changes the pain more than neck position does.
Conclusion
Shoulder impingement typically causes pain during a sideways arm lift between 60° and 120°. Night pain that wakes you and weakness without true tendon damage complete the early warning triad.
A hooked acromion or repetitive overhead activity narrows the subacromial space over time. The bursa swells first, then the tendons fray, then the cycle accelerates without intervention.
Most impingement resolves with physical therapy and one or two corticosteroid injections when caught early. Ignoring the pinch during overhead reach allows progression to rotator cuff tear which often requires surgery.
The treatment of postherpetic neuralgia in the elderly requires careful consideration, as age-related changes in the nervous system, comorbidities, and medication sensitivity make management more complex. Postherpetic neuralgia (PHN) is a chronic neuropathic pain condition that occurs after a shingles (herpes zoster) outbreak.
It can significantly affect quality of life, limiting mobility, sleep, and overall daily functioning. In older adults, PHN is not only more common but also more persistent and challenging to treat due to increased pain sensitivity and slower healing.
Many elderly patients live with PHN for months or even years, often experiencing burning, stabbing, or shooting pain along the nerve path affected by the original shingles rash. The goal of treatment is to relieve pain, improve function, prevent complications, and minimize adverse effects, particularly because elderly individuals are more susceptible to medication-related side effects.
This guide explores the most effective treatment strategies for postherpetic neuralgia in older adults, including pharmacologic and non-pharmacologic approaches, emerging therapies, and practical considerations for optimizing outcomes while minimizing risks.
Understanding Postherpetic Neuralgia in the Elderly
Postherpetic neuralgia occurs when nerve fibers damaged by the varicella-zoster virus fail to heal properly, leading to persistent pain after the shingles rash has resolved. The condition is more common in older adults, with incidence rising sharply after the age of 60. Age-related immune decline, slower nerve regeneration, and preexisting neuropathies contribute to prolonged and severe pain in this population.
The hallmark symptoms of PHN include:
- Burning, stabbing, or electric-like pain in the area of the previous rash
- Allodynia (pain from normally non-painful stimuli, like light touch or clothing)
- Hyperalgesia (heightened sensitivity to pain)
- Sleep disturbances due to persistent discomfort
- Reduced mobility and activity due to pain avoidance
Because PHN can be debilitating, effective management is critical. Uncontrolled pain can lead to depression, social withdrawal, and decreased quality of life in elderly patients.
Risk Factors and Challenges in the Elderly
Several factors make the treatment of postherpetic neuralgia in the elderly uniquely challenging. Age-related physiological changes, such as altered drug metabolism, decreased renal and hepatic function, and polypharmacy, increase the risk of adverse drug effects.
Cognitive impairment, frailty, and comorbid conditions like diabetes or cardiovascular disease further complicate management.
Other challenges include:
- Increased likelihood of severe PHN following shingles outbreaks in older adults
- Slower response to treatment and prolonged healing times
- Higher sensitivity to side effects of systemic medications such as dizziness, sedation, or orthostatic hypotension
- Difficulty adhering to complex medication regimens
Given these factors, treatment strategies must balance efficacy with safety, using individualized approaches that account for each patient’s overall health, comorbidities, and personal preferences.
Pharmacologic Treatments for Postherpetic Neuralgia
Medications remain the cornerstone of PHN management in older adults, targeting nerve pain, reducing discomfort, and improving functional outcomes. Selection of therapy depends on pain severity, patient comorbidities, potential side effects, and prior response to treatments.

First-Line Medications: Anticonvulsants
Anticonvulsants such as gabapentin and pregabalin are often the first-line pharmacologic treatment for postherpetic neuralgia in the elderly. These drugs modulate nerve excitability and reduce neuropathic pain signals in the central nervous system.
- Gabapentin: Effective in reducing PHN pain, especially in elderly patients. Dosing typically starts low to reduce the risk of dizziness or sedation, then titrated gradually. Benefits may take several days to weeks to manifest. Side effects can include drowsiness, balance issues, and peripheral edema.
- Pregabalin: Similar mechanism to gabapentin but with more predictable pharmacokinetics, making dosing easier. Often preferred when a rapid onset of pain relief is desired. Potential adverse effects include dizziness, somnolence, and weight gain.
Both medications require careful monitoring in elderly patients, particularly those with impaired renal function, due to increased risk of drug accumulation and toxicity.
Topical Therapies
Topical treatments provide localized pain relief with fewer systemic side effects, making them valuable for elderly patients. Common options include:
- Lidocaine 5% patches: Applied directly to the area of pain, these patches numb the affected nerve endings and reduce burning sensations. They are generally well-tolerated and suitable for frail patients.
- Capsaicin cream or patches: High-concentration capsaicin depletes substance P from nerve endings, decreasing pain signaling over time. Initially, it may cause a burning sensation, which can limit adherence in some elderly patients.
Topical agents are especially useful in patients who cannot tolerate systemic medications due to comorbidities or polypharmacy concerns.
Tricyclic Antidepressants (TCAs)
TCAs, such as amitriptyline and nortriptyline, are effective for PHN due to their ability to modulate pain pathways, though they carry higher risk of side effects in the elderly. They may improve mood and sleep in addition to reducing pain.
Common considerations include:
- Side effects: Dry mouth, constipation, urinary retention, sedation, and risk of cardiac arrhythmias.
- Dosing: Start at low doses and increase gradually, monitoring for anticholinergic effects or orthostatic hypotension.
- Suitability: Best for elderly patients without significant cardiac disease or cognitive impairment.
Due to these risks, TCAs are often reserved for patients who cannot achieve adequate relief with topical agents or anticonvulsants alone.
Opioids: When Other Treatments Fail
Opioids may be considered for severe, refractory PHN in the elderly, but they carry significant risks. Use is typically short-term and carefully monitored due to:
- Sedation and confusion, increasing fall risk
- Constipation and gastrointestinal complications
- Potential for dependency or misuse
- Interaction with other medications
If used, the lowest effective dose should be prescribed, with ongoing reassessment to minimize long-term harm.
Combination Therapy
Often, the best results in elderly patients come from combining therapies. For example, an anticonvulsant may be used alongside topical lidocaine or a low-dose TCA. Combination therapy targets multiple pathways of neuropathic pain while allowing lower doses of each medication, reducing the risk of adverse effects.
Combination strategies should be personalized, considering the patient’s comorbidities, renal and hepatic function, and cognitive status.
Non-Pharmacologic Treatments
Non-drug approaches play a crucial role in the treatment of postherpetic neuralgia in the elderly, particularly when medication tolerance is limited. These therapies focus on nerve modulation, physical support, and lifestyle adjustments.

Transcutaneous Electrical Nerve Stimulation (TENS)
TENS therapy uses low-level electrical currents to reduce nerve pain signals and improve comfort. It is non-invasive and generally well-tolerated by elderly patients. Proper electrode placement and session duration should be guided by a trained professional to optimize results.
Physical Therapy and Gentle Exercise
Physical therapy supports overall mobility, reduces stiffness, and improves functional outcomes. Gentle stretching, balance exercises, and low-impact activities help maintain muscle strength without exacerbating nerve pain. Exercise also improves circulation and reduces secondary complications from inactivity.
Cognitive Behavioral Therapy (CBT)
CBT can help elderly patients manage the emotional and psychological impact of chronic PHN pain. Techniques include relaxation training, coping strategies, and cognitive restructuring to reduce pain-related distress, sleep disruption, and depression.
Acupuncture and Complementary Therapies
Acupuncture and other complementary approaches may provide additional pain relief for some patients. While evidence varies, these options are often considered when conventional therapies provide incomplete relief. They carry minimal systemic side effects, making them suitable for older adults with multiple comorbidities.
Lifestyle Modifications
Simple lifestyle changes can enhance the effectiveness of other treatments. These include:
- Maintaining proper hydration and nutrition
- Practicing good sleep hygiene
- Avoiding triggers such as stress or excessive sun exposure (for shingles-related skin sensitivity)
- Using protective clothing to reduce skin irritation
These measures help reduce pain intensity and improve overall quality of life.
Emerging and Advanced Therapies
Research continues to explore new approaches for treating postherpetic neuralgia in the elderly. Some promising options include:
- Botulinum toxin injections: Targeted injections into affected areas reduce nerve pain signaling.
- Nerve blocks: Local anesthetic injections around affected nerves provide temporary relief for severe cases.
- Neuromodulation devices: Implanted devices or non-invasive stimulators modulate nerve activity and reduce pain perception.
While these treatments may not be first-line, they provide additional options for patients who do not respond adequately to traditional therapies.
Safety and Monitoring Considerations
Elderly patients require close monitoring due to age-related vulnerabilities and polypharmacy. Key safety considerations include:
- Regular assessment of renal and hepatic function when using systemic medications
- Monitoring for dizziness, sedation, or balance issues to prevent falls
- Gradual dose adjustments to minimize side effects
- Education on recognizing adverse reactions and reporting changes promptly
A multidisciplinary approach often yields the best outcomes, involving primary care physicians, pain specialists, pharmacists, and physical therapists.
Evaluating Treatment Success
Successful treatment of postherpetic neuralgia in the elderly is measured not only by pain reduction but also by improvements in function, sleep, and quality of life. Outcome measures include:
- Reduced pain intensity and frequency
- Improved daily mobility and activity levels
- Better sleep patterns
- Reduced dependence on multiple medications
- Enhanced mood and social engagement
Regular follow-up allows adjustments to therapy and ensures that benefits outweigh risks. Personalized treatment plans maximize comfort and safety for older adults.
Key Takeaways for Effective PHN Management
Treating postherpetic neuralgia in the elderly requires a comprehensive, individualized approach. Key takeaways include:
- Start with first-line therapies such as anticonvulsants and topical agents.
- Combine pharmacologic and non-pharmacologic treatments to target multiple pain pathways.
- Monitor closely for side effects, drug interactions, and changes in overall health.
- Prioritize therapies that preserve function, minimize systemic risk, and maintain quality of life.
- Consider advanced or emerging therapies for refractory cases.
- Use lifestyle modifications and supportive care to enhance treatment effectiveness.
These strategies help ensure that elderly patients experience meaningful relief while minimizing risks and complications.
Conclusion
The treatment of postherpetic neuralgia in the elderly is multifaceted, balancing efficacy, safety, and quality of life. While medications like gabapentin, pregabalin, and topical lidocaine provide first-line relief, combination therapy with non-pharmacologic measures often yields the best outcomes.
Elderly patients are particularly vulnerable to side effects, polypharmacy issues, and comorbidities, making individualized care and close monitoring essential. Lifestyle modifications, physical therapy, cognitive behavioral therapy, and complementary therapies can further enhance outcomes and reduce reliance on medications.
Ultimately, effective management focuses not just on pain reduction but on preserving function, improving sleep, supporting mental health, and enhancing overall quality of life. By understanding the range of available treatments, carefully considering patient-specific factors, and employing a multidisciplinary approach, healthcare providers can help elderly patients navigate postherpetic neuralgia safely and effectively.
Nerve pain from shingles years later is primarily caused by long-term damage and hypersensitivity of the nerves triggered by the varicella-zoster virus, and relief options include medications, topical treatments, nerve blocks, and self-care pain management strategies. This lingering condition, known as postherpetic neuralgia, can persist long after the shingles rash has healed because the affected nerves continue sending abnormal pain signals to the brain.
This article covers how shingles leads to long-term nerve damage, why pain can persist or return years later, common symptoms, treatment options, and prevention and risk reduction strategies. It also briefly discusses risk factors and when to seek medical help for ongoing or worsening pain.

What Is Happening in the Nerves?
Shingles is caused by the varicella-zoster virus, the same virus responsible for chickenpox. After a person recovers from chickenpox, the virus does not fully leave the body. Instead, it remains dormant in nerve tissue for years - sometimes decades - and can reactivate later in life as shingles when immunity weakens.
During a shingles outbreak, several changes occur in the nervous system:
- The virus increases inflammation and directly damages nerve fibers
- Affected nerves become overly sensitive, irritated, or start misfiring
- Even after the skin rash heals, pain signals can continue to fire abnormally
In some cases, this damage leads to postherpetic neuralgia (PHN), where the nervous system becomes “stuck” in a heightened pain state.
As a result, damaged nerves may keep sending distorted or amplified pain signals to the brain, even in the absence of an active infection. This can produce persistent sensations such as burning, stabbing, tingling, or electric-shock-like pain long after the shingles rash has resolved.
Why Nerve Pain Can Appear Years Later
In some people, nerve pain linked to shingles does not fully disappear after the initial infection and may return or become noticeable again years later. This delayed or persistent pain is usually related to how the virus affected the nerves and how the nervous system continues to respond over time.
1. Delayed Nerve Irritation or Sensitization
Damaged nerves may remain unstable even after healing. Over time, normal wear, aging, or minor inflammation can trigger renewed sensitivity or pain signals.
2. Incomplete Nerve Healing
Some nerve fibers do not fully regenerate after shingles damage. This can leave behind weakened or scarred nerves that intermittently misfire and cause pain later on.
3.Central Sensitization (Brain and Spinal Cord Changes)
The nervous system can become “rewired” to interpret normal sensations as pain. Even after the infection is gone, the brain may continue to overreact to signals from the affected area.
4. Triggering Factors Years Later
Factors such as aging, stress, illness, or a weakened immune system can reactivate or amplify dormant nerve sensitivity. These triggers may cause old nerve pain to resurface or worsen.
5. Residual Nerve Damage From Past Infection
In some cases, the original shingles episode leaves long-lasting nerve injury that only becomes noticeable when the body is under strain or natural degeneration occurs with age.
Overall, late-appearing nerve pain after shingles is usually the result of lingering nerve damage combined with changes in how the nervous system processes pain over time.
What Nerve Pain Feels Like
Nerve pain after shingles can vary widely from person to person, but it is often described as unusual, intense, and difficult to ignore. It tends to affect the same area where the original shingles rash appeared and can range from mild discomfort to severe, disabling pain.
1. Burning or Hot Sensation
Many people describe it as a constant burning feeling, similar to having the skin on fire. This sensation can persist even without any visible skin changes.
2. Sharp, Stabbing, or Electric Shock Pain
The pain may come in sudden bursts that feel like stabbing or electric shocks. These episodes can be brief but extremely intense.
3. Deep Aching or Throbbing Pain
Some experience a persistent, deep ache that feels like it is coming from within the nerves or muscles. This type of pain can be constant and exhausting over time.
4. Extreme Sensitivity to Touch (Allodynia)
Even light contact, such as clothing or a gentle breeze, can trigger significant pain. This heightened sensitivity makes everyday activities uncomfortable.
5. Numbness Mixed With Pain
In some cases, areas of the skin may feel numb while still producing pain signals. This confusing mix occurs because damaged nerves send inconsistent messages to the brain.
Nerve pain from shingles is often complex and can combine multiple sensations, making it one of the more challenging types of chronic pain to live with.
Relief Options and Treatment Strategies
Managing nerve pain after shingles often requires a combination of medical treatments and supportive therapies. Because the pain is nerve-related rather than purely skin-deep, approaches usually focus on calming overactive nerve signals and improving overall comfort.

1. Prescription Medications
Doctors often prescribe nerve-targeting medications such as gabapentin or pregabalin to reduce abnormal nerve firing. Certain antidepressants like amitriptyline or nortriptyline may also help regulate pain signals and improve sleep.
2. Topical Treatments (Skin-Based Relief)
Topical options such as lidocaine patches can numb the affected area and provide temporary relief from localized pain. Capsaicin cream or patches may also help by gradually reducing the sensitivity of nerve endings over time.
3. Advanced Medical Procedures
For more severe or persistent cases, treatments like nerve blocks or steroid injections may be used to interrupt pain signaling. In rare cases, procedures such as spinal cord stimulation are considered when other options are not effective.
4. Non-Medication Approaches
Therapies such as physical therapy, gentle movement, and acupuncture may help reduce nerve sensitivity and improve function. Mind-body techniques like relaxation exercises and meditation can also assist in managing pain perception.
5. Lifestyle Support
Good sleep habits, stress management, and regular low-impact exercise can help stabilize the nervous system and reduce flare-ups. A balanced diet and overall health maintenance also support nerve recovery and resilience.
In summary, effective relief often comes from combining multiple strategies rather than relying on a single treatment. Working with a healthcare provider helps tailor the right mix of options based on pain severity and individual response.
Can It Go Away?
Post-shingles nerve pain (postherpetic neuralgia) can improve over time, but the course varies widely from person to person. Some people experience gradual relief within months, while others may have symptoms that last for years.
1. Yes, in many people it gradually improves
Nerves can slowly recover and become less sensitive over time, leading to reduced pain intensity. This is more likely when nerve damage is mild or when treatment begins early.
2. Some people experience long-term or chronic pain
If nerve damage is more severe, pain may persist for years or become a long-term condition. In these cases, symptoms are usually managed rather than fully cured.
3. Pain may come and go over time
Even when not constant, nerve pain can flare up due to stress, illness, or fatigue. These episodes often become less frequent or less intense over time.
4. Treatment can significantly improve outcomes
Medications, therapies, and lifestyle changes can reduce pain and improve nerve function. While not always eliminating pain completely, they often make it much more manageable.
Nerve pain after shingles can go away for some people, especially with mild nerve damage and proper care. However, for others it may persist long-term, making ongoing management and treatment important for maintaining quality of life.
When to See a Doctor
Nerve pain after shingles can sometimes be managed at home, but persistent or worsening symptoms may require medical attention. Early evaluation can help rule out other conditions and improve treatment outcomes.
1. Pain Lasts for Weeks or Months After Shingles
If nerve pain continues long after the rash has healed, it may indicate postherpetic neuralgia. A doctor can help confirm the diagnosis and recommend appropriate treatment.
2. Pain Is Getting Worse Instead of Improving
Worsening pain over time may suggest ongoing nerve irritation or another underlying issue. Medical assessment is important to adjust or start treatment early.
3. Pain Affects Sleep or Daily Activities
When discomfort interferes with rest, work, or basic functioning, it should be evaluated. Proper treatment can significantly improve quality of life.
4. New Neurological Symptoms Appear
Symptoms like muscle weakness, spreading numbness, or unusual sensations should be checked promptly. These may indicate additional nerve involvement or other conditions.
You should see a doctor if nerve pain persists, worsens, or begins to interfere with daily life. Early treatment can help manage symptoms more effectively and prevent long-term discomfort.
Prevention and Risk Reduction
Proactive measures are the most effective defense against the long-term neurological complications associated with the shingles virus. By focusing on both clinical prevention and early intervention, individuals can significantly lower their chances of developing chronic nerve pain.
1. Vaccination Protocol
The most effective preventive measure is the recombinant zoster vaccine, which is over 90% effective at preventing shingles and its subsequent nerve complications in older adults.
2. Early Antiviral Intervention
Starting prescription antiviral medications within 72 hours of the initial rash appearing can limit nerve damage and drastically reduce the duration of the infection.
3. Immune System Support
Maintaining a robust immune system through balanced nutrition and stress management helps keep the dormant virus suppressed within the nerve tissues.
4. Prompt Pain Management
Addressing acute pain aggressively during the initial outbreak may prevent the nervous system from becoming "sensitized," which often leads to long-term neuralgia.
Taking these steps not only reduces the likelihood of an initial outbreak but also ensures that if shingles does occur, the impact on your long-term quality of life is minimized. Consistently monitoring your health and staying current with recommended immunizations remains the gold standard for risk reduction.
Key Takeaway
Nerve pain after shingles is caused by lasting damage and increased sensitivity in nerves affected by the varicella-zoster virus, which can continue to send pain signals even long after the skin has healed. Relief typically involves a mix of medications, topical therapies, medical procedures, and supportive lifestyle changes that work together to calm nerve activity.
For some people, the pain gradually improves over time, while for others it may persist and require long-term management. With appropriate treatment and consistent care, symptoms can often be significantly reduced, leading to better comfort and improved daily living.
After trigger point injections, you should avoid intense physical activity, aggressive massage, heat application, alcohol, and ignoring post-treatment instructions to ensure safe and effective recovery. These precautions help prevent unnecessary irritation, reduce the risk of complications, and allow the treated muscles to heal properly so you can get the full benefit of the procedure.
In this article, we’ll briefly explain what trigger point injections (TPI) are, what to do instead for proper recovery, expected healing time, and common side effects. We’ll also cover when to see a doctor, tips to maximize results, and simple lifestyle changes to help prevent future trigger points. Let's look at what not to do after trigger point injections for safe recovery.
What Is a Trigger Point Injection?
A trigger point injection is a medical treatment used to relieve pain caused by tight, sensitive knots in muscles, known as trigger points. It involves inserting a small needle directly into the affected area to deliver a local anesthetic, saline, or sometimes a corticosteroid to relax the muscle and reduce pain.
These injections are commonly used for conditions like muscle tension, myofascial pain, and tension headaches. The procedure is quick, minimally invasive, and often provides relief by improving blood flow and allowing the muscle to return to its normal function.
What Not to Do After Trigger Point Injections
Proper aftercare is essential to ensure you get the best results from trigger point injections and avoid unnecessary complications. Knowing what to avoid can help reduce irritation, support healing, and improve overall recovery.

1. Avoid Intense Physical Activity
Strenuous exercise or heavy lifting can strain the treated muscles and delay healing. It’s important to give your body time to recover before returning to high-impact activities.
2. Don’t Massage the Area Aggressively
Applying deep pressure or using massage tools on the injection site can increase inflammation and discomfort. Gentle movement is fine, but avoid anything that puts excessive force on the area.
3. Avoid Applying Heat Immediately
Using heat too soon after the injection may worsen swelling and irritation. Instead, allow the area to settle first, and consider cold therapy if needed.
4. Don’t Ignore Unusual Symptoms
While mild soreness is normal, worsening pain or signs of infection should not be overlooked. Contact a healthcare provider if symptoms seem unusual or persist longer than expected.
5. Avoid Alcohol and Dehydration
Alcohol can interfere with the healing process and may increase inflammation. Staying well-hydrated supports muscle recovery and overall healing.
6. Don’t Skip Post-Treatment Instructions
Your provider’s aftercare guidelines are tailored to your condition and recovery needs. Ignoring them can reduce the effectiveness of the treatment and prolong discomfort.
Avoiding these common mistakes after trigger point injections can make a significant difference in your recovery. Following proper care guidelines helps ensure better results and reduces the risk of complications.
What You Should Do Instead
Taking the right steps after trigger point injections is just as important as avoiding certain activities. Proper care can enhance healing, reduce discomfort, and help you get the most out of your treatment.
1. Stay Hydrated
Drinking plenty of water helps flush out toxins and supports muscle recovery. Proper hydration also improves circulation, which can aid in reducing soreness and stiffness.
2. Engage in Light Movement
Gentle movements like walking or easy stretching can help prevent stiffness without overloading the treated muscles. Keeping the body moving promotes blood flow and supports faster healing.
3. Use Cold Therapy if Needed
Applying a cold pack to the injection site can help reduce inflammation and numb soreness. Be sure to use it in short intervals to avoid skin irritation.
4. Gradually Return to Normal Activities
Ease back into your regular routine instead of jumping into intense activities right away. This gradual approach helps your muscles adapt and prevents re-injury.
5. Follow a Physical Therapy Plan
If recommended, physical therapy can strengthen muscles and address underlying issues causing trigger points. Consistency with exercises can improve long-term outcomes.
6. Maintain Good Posture and Ergonomics
Pay attention to your posture, especially during work or daily activities. Proper alignment reduces strain on muscles and helps prevent trigger points from recurring.
Following these positive recovery steps can significantly improve the effectiveness of your trigger point injections. A balanced approach of rest, gentle activity, and healthy habits supports long-term relief and muscle health.
Recovery Checklist: At a Glance
This checklist provides a quick overview of what to do and avoid after trigger point injections for safe recovery.
| Category | Do | Don't |
| Physical Activity | Engage in light movement and gentle stretching | Perform intense workouts or heavy lifting |
| Massage | Use gentle touch if needed | Apply deep pressure or massage tools on the injection site |
| Temperature | Apply cold packs if sore | Use heat immediately after injection |
| Hydration & Alcohol | Stay hydrated | Drink alcohol within 24–48 hours |
| Symptoms | Monitor for mild soreness | Ignore worsening pain, swelling, or signs of infection |
| Post-Treatment Instructions | Follow healthcare provider's advice | Skip instructions or ignore follow-up care |
Quick Tips:
- Gradually return to normal activities instead of rushing.
- Maintain good posture and ergonomics during daily activities.
- Consider physical therapy or exercises recommended by your provider.
- Track symptoms to report any unusual changes promptly.
How Long Does Recovery Take?
Recovery after trigger point injections varies depending on the individual and the severity of muscle tension. Most people experience gradual improvement within days to weeks.
- Immediate soreness (24–72 hours): Mild discomfort or tenderness at the injection site is common during the first few days. This usually subsides on its own without any special treatment.
- Pain relief onset (within a few days): Many people begin to notice reduced muscle tension and pain shortly after the procedure. Relief may feel gradual as the muscle starts to relax.
- Full benefit (1–2 weeks): The maximum effect of the injection is typically felt within one to two weeks. By this time, muscle function and comfort should significantly improve.
While some relief can be felt quickly, full recovery takes a bit more time. Being patient and following aftercare guidelines can help ensure the best outcome.
Common Side Effects to Expect
After trigger point injections, some mild side effects are normal as your muscles respond to the treatment. Most are temporary and resolve without intervention.
- Local soreness or tenderness: The injection site may feel sore for a day or two. This usually improves with rest or light movement.
- Minor bruising: Small bruises can appear around the injection site. They typically fade within a few days.
- Temporary numbness or weakness: Some people may experience brief numbness or reduced muscle strength. These effects usually resolve quickly as the anesthetic wears off.
Mild discomfort, bruising, and temporary numbness are common and expected. If any symptoms persist or worsen, it’s important to contact your healthcare provider.
When to Contact a Doctor
While most side effects after trigger point injections are mild, it’s important to know when professional medical advice is necessary. Prompt attention can prevent complications and ensure proper healing.

1. Persistent or Worsening Pain
If the pain at the injection site increases instead of gradually improving, contact your doctor. This may indicate an underlying issue or complication that needs evaluation and prompt management.
2. Signs of Infection
Redness, swelling, warmth, or pus around the injection site should not be ignored. Early medical attention can prevent the infection from worsening or spreading.
3. Difficulty Breathing or Severe Swelling
Sudden breathing problems or rapid swelling around the face or throat require urgent medical care. These could be signs of a serious allergic reaction or other critical complication.
4. Allergic Reactions
Symptoms such as hives, rash, itching, or sudden swelling should be addressed immediately. Severe reactions may require emergency treatment to prevent life-threatening issues.
While mild soreness is expected, any unusual or worsening symptoms should be reported to a healthcare provider. Timely intervention helps ensure a safe and effective recovery.
Tips to Maximize Treatment Effectiveness
Following certain practices after trigger point injections can help you achieve the best possible results and support long-term relief. These strategies complement the injection by addressing underlying muscle issues.
1. Combine Treatment With Physical Therapy
Physical therapy helps strengthen muscles and prevent recurrence. Consistent exercises can improve overall outcomes.
2. Maintain Good Posture
Proper posture reduces strain on muscles and prevents new trigger points from forming. Be mindful during work and daily activities.
3. Address Underlying Causes
Identify factors like stress, poor ergonomics, or repetitive strain that contribute to muscle tension. Making adjustments can reduce future flare-ups.
4. Stay Consistent With Follow-Up Care
Attend all recommended appointments and follow medical advice. This ensures ongoing monitoring and optimal recovery.
Integrating these tips into your routine can enhance the effectiveness of trigger point injections and promote lasting relief. Consistency and awareness are key to long-term muscle health.
Lifestyle Changes to Prevent Trigger Points
Adopting certain lifestyle habits can help prevent trigger points from recurring and support overall muscle health. Consistent attention to posture, movement, and stress management is key.
1. Stretch Regularly
Incorporate daily stretches to maintain flexibility and reduce muscle tension. Focus on areas prone to trigger points.
2. Take Breaks From Prolonged Sitting
Move around periodically to prevent stiffness and maintain circulation. Simple posture adjustments can make a big difference.
3. Improve Workstation Ergonomics
Ensure your desk, chair, and monitor setup reduce strain on muscles. Proper ergonomics prevent repetitive stress injuries.
4. Manage Stress Through Relaxation Techniques
Practice mindfulness, deep breathing, or yoga to relieve tension. Stress reduction can lower muscle tightness and trigger points.
5. Stay Physically Active With Low-Impact Exercises
Engage in activities like walking, swimming, or cycling to keep muscles strong and flexible. Regular activity reduces the likelihood of knots forming.
These lifestyle changes support long-term muscle health and help prevent trigger points. Combining movement, posture awareness, and stress management can greatly reduce the risk of recurrence.
Final Thoughts
Trigger point injections can provide significant relief from muscle pain and improve mobility, but their effectiveness depends heavily on proper aftercare. Avoiding strenuous activity, heat, deep massage, and alcohol, while adhering to your provider’s instructions, is crucial for a smooth recovery and minimizing complications.
Pairing these precautions with healthy habits like staying hydrated, gentle movement, maintaining good posture, and making lifestyle adjustments can enhance the benefits of the treatment and help prevent future trigger points. Patience, consistency, and mindful self-care are essential for long-lasting relief and overall muscle health.
A stellate ganglion block injects local anesthetic near a nerve bundle in the lower neck. This procedure temporarily interrupts overactive sympathetic signals that drive chronic pain, post-traumatic stress, and long COVID symptoms.
The stellate ganglion sits along the spinal column and acts as a relay station for fight-or-flight responses. When this nerve cluster fires too aggressively, it can cause persistent arm pain, insomnia, and a racing heart.
One injection often produces immediate warmth and redness in the affected hand. That physical sign confirms the block successfully relaxed the nerve's grip on blood vessels and sweat glands. Let's look at stellate ganglion blocks explained , what to expect and how they work.
What Is a Stellate Ganglion Ganglion?
The stellate ganglion is a collection of nerve cell bodies located at the level of the lower neck, specifically between the C7 and T1 vertebrae. This structure measures roughly 1 centimeter in size and resembles a star, which gave it the name "stellate" from the Latin word for star.
- Location and Anatomy
The ganglion sits just in front of the longus colli muscle and behind the carotid artery and internal jugular vein. Its position near the esophagus and trachea explains why a block can temporarily cause hoarseness or a droopy eyelid.
- The Sympathetic Chain Connection
This nerve cluster belongs to the sympathetic nervous system, which controls involuntary functions like heart rate and blood vessel constriction. The stellate ganglion specifically sends signals to the head, neck, arms, and upper chest.
What the Stellate Ganglion Does
- It constricts blood vessels in the upper limb and face
- It controls sweating on the same side of the body
- It dilates the pupil and lifts the eyelid
- It helps regulate heart rate through nerve branches to the heart
Each of these functions serves a protective purpose during physical threat or injury. When the ganglion fires too often without a real threat, those same actions cause problems like cold hands, facial sweating, or a racing pulse.
How the Block Actually Works
The procedure deposits a small volume of local anesthetic, usually lidocaine or bupivacaine, directly around the stellate ganglion. This anesthetic temporarily stops the nerve from sending electrical signals along the sympathetic chain.
- The Mechanism of Nerve Blockade
Local anesthetic molecules enter the nerve cell membrane and bind to sodium channels. This binding prevents sodium from entering the cell, which blocks the action potential from traveling further.
Without a propagating action potential, the ganglion cannot relay pain signals or vasoconstrictor commands to the upper body. The result is a temporary chemical shutdown of that specific nerve cluster.
- What Resetting Means Physiologically
A successful block interrupts the feedback loop of chronic sympathetic overactivity. The nerve does not get damaged or destroyed, only silenced for several hours.
After the anesthetic wears off, the ganglion often resumes a lower baseline firing rate. This reset effect can last weeks or months in some patients.
- Immediate Physical Changes After Injection
Blood vessels in the blocked side dilate, which causes visible redness and measurable warmth in the hand and arm. Sweating stops on that same side of the face and upper limb.
The pupil constricts slightly and the upper eyelid droops, a combination called Horner syndrome. These signs confirm accurate anesthetic placement and predict a better clinical outcome.
Who Usually Gets This Injection
The stellate ganglion block has regulatory approval for several pain conditions but remains off-label for most psychiatric uses. A pain management physician or anesthesiologist typically determines candidacy based on symptom pattern and prior treatment failures.
- Complex Regional Pain Syndrome (CRPS)
CRPS patients experience burning pain, swelling, and skin color changes in one arm after a minor injury or surgery. The block can interrupt the sympathetically maintained pain that drives this condition.
A positive response to a diagnostic block predicts good outcomes from a series of therapeutic blocks. Many CRPS patients receive three injections spaced two weeks apart for optimal relief.
- Post-Traumatic Stress Disorder (PTSD)
Military veterans and civilian trauma survivors with PTSD have shown symptom reduction after stellate ganglion block. The proposed mechanism involves resetting an overactive amygdala response to non-threatening stimuli.
Clinical studies report decreased hypervigilance, fewer nightmares, and lower anxiety scores post-injection. The effect appears within one hour and can last several weeks.
- Long COVID and Post-Viral Syndromes
Patients with long COVID often present with inappropriate tachycardia, temperature dysregulation, and fatigue. These symptoms mirror sympathetic overdrive and respond to stellate ganglion blockade in small case series.
Early data suggests the block may reduce brain fog and improve sleep quality. Research continues to define which long COVID subgroups benefit most.
- Phantom Limb Pain and Herpes Zoster
Amputees who feel burning or cramping in a missing limb sometimes gain relief from this injection. The same procedure can reduce the shooting pain of post-herpetic neuralgia after shingles.
These conditions share a component of sympathetically maintained pain. The block offers an alternative when oral medications fail or cause intolerable side effects.
What Happens Right Before the Procedure
A pre-procedure evaluation includes a review of current medications and a brief neurological exam. The physician asks about any history of bleeding disorders or allergic reactions to local anesthetics.
- Medication Adjustments
Blood thinners such as warfarin, apixaban, or clopidogrel require a temporary hold before the injection. The physician provides specific stop dates based on each drug's half-life.
Non-steroidal anti-inflammatory drugs like ibuprofen or naproxen may also need a pause for three days. Aspirin at low doses for heart protection often continues with physician approval.
- Positioning and Monitoring
The patient lies flat on an examination table with the head turned slightly away from the injection side. A small roll or pillow supports the neck to expose the anterior cervical spine.
An intravenous line is placed for emergency access although serious complications remain rare. Standard monitors track heart rate, blood pressure, and oxygen saturation throughout the brief procedure.
- Imaging Guidance Setup
A high-frequency ultrasound probe sits on the side of the neck to visualize the carotid artery, thyroid, and nerve roots. The physician identifies the stellate ganglion at the C7 level near the longus colli muscle.
Fluoroscopy, a live X-ray technique, serves as an alternative when ultrasound cannot clearly show bony landmarks. Both methods confirm needle tip position before anesthetic injection.
Step by Step During the Injection
The skin over the lower neck receives a small wheal of lidocaine to numb the needle entry site. This superficial injection burns for several seconds then fades to complete numbness.
- Needle Placement
A three-inch, 25-gauge needle advances through the numbed skin toward the stellate ganglion. The physician watches the needle tip on the ultrasound screen or fluoroscope to avoid the carotid artery and vertebral vessels.
Gentle aspiration confirms the needle has not entered a blood vessel. A small amount of contrast dye may be injected under X-ray to verify spread around the ganglion.
- The Anesthetic Injection
5 to 10 milliliters of local anesthetic, usually lidocaine 1% or ropivacaine 0.2%, passes slowly through the needle. The patient feels deep pressure but not sharp pain during the injection.
The medication spreads along the fascial plane surrounding the sympathetic chain. A successful injection produces a visible change in tissue appearance on ultrasound.
- Sensations During the Injection
A warm flush travels down the arm on the injected side within 30 to 60 seconds. The hand may feel heavy or tingly as blood vessels dilate.
Some patients report a metallic taste in the mouth or a feeling of a lump in the throat. These sensations pass within a few minutes and do not indicate any problem.
- Duration of the Needle Procedure
The entire needle placement and injection process takes less than 10 minutes from start to finish. The patient remains awake and can report any unusual symptoms immediately.
Right After the Block What You Will Notice
The patient stays in a recovery area for 15 to 30 minutes after the injection. A nurse checks vital signs and monitors for any signs of local anesthetic toxicity or allergic reaction.
- Horner Syndrome Signs
The upper eyelid on the injected side droops slightly, a condition called ptosis. The pupil becomes smaller than the other side, which is miosis.
These two findings together confirm sympathetic blockade of the eye and face. The changes look concerning but cause no harm to vision or eye function.
- Voice and Throat Changes
The recurrent laryngeal nerve sits close to the stellate ganglion and may catch some anesthetic spread. This produces a hoarse or breathy voice that lasts 1 to 2 hours.
Some patients feel a lump in the throat or notice difficulty swallowing saliva. These symptoms resolve completely as the anesthetic wears off.
- Arm and Hand Findings
The injected side arm and hand turn pink or red from increased blood flow. The skin temperature rises by 1°C to 3°C compared to the other arm.
Sweating stops completely on the palm and forearm of the treated side. Patients often describe the arm as feeling warm, heavy, or slightly numb.
- Timeline for Resolution
Horner syndrome typically fades within 2 to 4 hours after the injection. The hoarse voice usually clears within 90 minutes.
The increased blood flow and warmth can persist for several hours to several days. This prolonged effect indicates a successful and durable nerve blockade.
Possible Side Effects and Risks
Most side effects from a stellate ganglion block are temporary and relate to the spread of local anesthetic to nearby structures. Serious complications occur in fewer than 1% of procedures when performed with imaging guidance.
- Common Temporary Side Effects
Hoarseness from recurrent laryngeal nerve block affects approximately 30% of patients. This resolves completely within 1 to 2 hours without any treatment.
Difficulty swallowing or a sensation of food sticking in the throat occurs less frequently. Patients should sip liquids slowly until normal swallowing returns.
Temporary Horner syndrome, including droopy eyelid and small pupil, happens in nearly every successful block. These signs reverse as the anesthetic wears off.
- Injection Site Issues
Bleeding under the skin at the needle entry point produces a small bruise that fades within 1 week. A tiny collection of blood called a hematoma may feel firm to the touch but resolves on its own.
Infection at the needle site presents as increasing redness, warmth, and tenderness after the first day. Oral antibiotics treat this rare complication effectively when caught early.
- Rare But Serious Risks
Seizure from accidental injection of local anesthetic into a blood vessel requires immediate treatment with intravenous lipid emulsion. Physicians prepare this rescue medication before every nerve block procedure.
Pneumothorax, or a punctured lung, occurs when the needle goes too deep and enters the pleural space. This complication causes chest pain and shortness of breath and requires chest tube placement.
Spinal cord injury or epidural spread of anesthetic is extraordinarily rare with ultrasound guidance. Permanent nerve damage has been reported but only in case reports spanning several decades.
Dorsal Root Ganglion Stimulation Procedure: How It Works
The stellate ganglion block offers a temporary reset for an overactive sympathetic nerve cluster in the neck. Patients with CRPS, PTSD, or long COVID may find significant relief from a single injection or a short series of three.
A related but distinct procedure targets a different nerve structure called the dorsal root ganglion. The dorsal root ganglion lies inside the spinal canal and controls sensory signals rather than sympathetic fight-or-flight responses.
While the stellate ganglion block numbs nerves outside the spine, dorsal root ganglion stimulation modulates pain signals at their spinal entry point. Both interrupt pain pathways in different ways, and patients who fail one may still respond to the other.
Recovery after a sacroiliac joint injection is usually quick, with most patients returning to normal activities within a few days, though full pain relief may take one to three weeks. The exact timeline depends on your body, the severity of your condition, and how well you follow post-procedure care instructions.
Many patients are surprised by how manageable the recovery process is, especially when they know what to expect ahead of time. In most cases, sacroiliac joint injection recovery time is short, but the full benefits develop gradually as inflammation decreases and healing progresses.
Understanding this timeline helps you plan daily activities, avoid unnecessary strain, and feel more confident about the procedure. This guide breaks down each stage of recovery, key influencing factors, and practical ways to support better outcomes.
What Is a Sacroiliac Joint Injection and Why Is It Done?
The sacroiliac joint connects the lower spine to the pelvis and plays a key role in absorbing shock and stabilizing movement. When this joint becomes inflamed or irritated, it can lead to persistent lower back and hip pain that may radiate into the legs.
A sacroiliac joint injection is a minimally invasive procedure used to diagnose or treat this pain. The injection typically contains a combination of a local anesthetic and a corticosteroid.
The anesthetic provides immediate but temporary relief, while the steroid works over time to reduce inflammation. Doctors often use imaging guidance to ensure the medication is delivered precisely into the joint space.
A sacroiliac joint injection serves both as a diagnostic tool and a targeted treatment for chronic lower back pain.
Conditions That May Require an SI Joint Injection
Several underlying issues can lead to sacroiliac joint pain. These include sacroiliitis, which is inflammation of the joint, and degenerative arthritis that develops over time. Injuries, such as falls or car accidents, can also disrupt the joint’s stability.
Pregnancy is another contributing factor due to hormonal changes that loosen ligaments around the pelvis. In some cases, pain originates from abnormal movement patterns that strain the joint repeatedly. Identifying the cause helps determine whether an injection is the right solution.
What Happens During the Procedure
The procedure is usually performed in an outpatient setting and takes less than 30 minutes. Patients lie face down while a physician uses fluoroscopy or CT imaging to guide a needle into the sacroiliac joint. After confirming proper placement, the medication is injected.
Most patients experience minimal discomfort during the process, especially when they understand what to expect from a pain management doctor before and during the procedure.
You may feel slight pressure or a brief stinging sensation, but sedation is rarely required. Once completed, patients are monitored briefly before being allowed to go home the same day.
Sacroiliac Joint Injection Recovery Time Explained
Recovery after the injection happens in stages, beginning immediately after the procedure and continuing over the following weeks. While many patients feel some relief right away due to the anesthetic, this effect wears off within hours.
The steroid component takes longer to reduce inflammation and provide lasting results. It is normal to experience mild soreness at the injection site, which typically resolves within a day or two.
Some patients may even notice a temporary increase in pain before improvement begins. This is part of the body’s response to the injection and usually subsides quickly.
Recovery after an SI joint injection is typically fast, but meaningful pain relief often builds gradually over several days.
Immediate Post-Procedure Recovery (First 24 Hours)
During the first day, you may feel numbness or weakness in the lower back or legs due to the anesthetic. This is temporary and should fade within a few hours.
Mild tenderness at the injection site is common and can be managed with rest. Patients are usually advised to avoid strenuous activity during this period and follow guidelines on what to avoid after a pain injection to prevent unnecessary irritation.
Light walking is acceptable, but heavy lifting or intense exercise should be postponed. Along with rest and ice application, you can also improve comfort during recovery by adopting proper sleeping positions for sacroiliac joint pain, which help reduce strain on the joint.
Short-Term Recovery (2 to 7 Days)
As the anesthetic wears off, some patients experience a brief return of pain. This can feel discouraging but is expected. The steroid medication begins working during this phase, gradually reducing inflammation in the joint.
Most people can resume normal daily activities within a couple of days. However, it is wise to ease back into physical routines rather than jumping in at full intensity. Paying attention to how your body responds is key to avoiding setbacks.
Long-Term Results (1 to 3 Weeks)
By the end of the first week, many patients begin to notice significant improvement in their symptoms. Pain levels decrease, mobility improves, and daily tasks become easier. Full benefits are often felt within two to three weeks.
If relief is minimal or short-lived, your doctor may reassess the diagnosis or recommend additional treatments. In some cases, repeat injections or physical therapy may be part of a broader care plan.
Common Side Effects During Sacroiliac Joint Injection Recovery
Understanding what your body might experience after the procedure helps reduce anxiety and ensures you respond appropriately to normal symptoms. While sacroiliac joint injections are generally safe, mild side effects are fairly common and typically short-lived.
These reactions are part of the body’s natural response to both the injection itself and the medication used. Most side effects occur within the first few days and gradually fade without intervention.
However, knowing the difference between expected discomfort and something that needs medical attention is important. Patients who are well-informed tend to recover more confidently and avoid unnecessary worry.
Most side effects after an SI joint injection are mild, temporary, and resolve within a few days without treatment.
Common Side Effects You May Experience
Here are the most frequently reported post-injection symptoms:
- Soreness at the Injection Site
Mild pain or tenderness where the needle was inserted is the most common complaint. This usually improves within 24 to 48 hours and can be managed with ice packs.
- Temporary Increase in Pain
Some patients experience a short-term flare-up before the steroid begins working. This can last a few days but is not a cause for concern.
- Numbness or Weakness
The anesthetic used during the injection may cause temporary numbness in the lower back or legs. This effect typically wears off within a few hours.
- Mild Swelling or Bruising
Slight swelling or bruising at the injection site may occur but generally resolves quickly.
- Headache or Fatigue
A small number of patients report feeling tired or developing a mild headache after the procedure.
- Facial Flushing from Steroids
Corticosteroids can sometimes cause temporary warmth or redness in the face, which fades within a day or two.
When Side Effects May Require Attention
Although rare, certain symptoms should not be ignored. Severe pain that worsens over time, signs of infection such as fever or redness, or prolonged numbness should be evaluated by a healthcare provider.
A 2020 review published in Pain Physician Journal found that serious complications from joint injections are uncommon, occurring in less than 1 percent of cases. This reinforces that most recovery experiences are straightforward and manageable.
Being aware of these potential side effects allows you to stay calm and focused during recovery. It also helps you distinguish between normal healing and situations that require medical input.
Factors That Affect Recovery Time
Not all patients recover at the same pace, especially since underlying conditions and the causes of lower back and hip pain can vary from person to person.
Several factors influence how quickly you feel better and how long the relief lasts. Understanding these variables can help set realistic expectations.
Your overall health plays a major role in recovery. Individuals with chronic conditions or inflammation elsewhere in the body may take longer to respond. Age, fitness level, and previous injuries also contribute to healing speed.
Recovery time varies because each patient’s condition, lifestyle, and response to treatment are unique.
- Personal Health and Medical History
Patients with conditions such as arthritis or obesity may experience slower improvement due to ongoing joint stress. Previous lower back injuries can also complicate recovery by affecting surrounding structures.
A 2022 report from the American Academy of Orthopaedic Surgeons noted that patients with multiple musculoskeletal conditions often require longer recovery periods and more comprehensive treatment plans.
- Activity Level After the Procedure
How you move after the injection matters. Too much rest can lead to stiffness, while overexertion can aggravate the joint. Finding a balance between gentle movement and adequate rest supports healing.
Gradual reintroduction of activity is usually recommended. Walking, stretching, and low-impact exercises can help maintain mobility without placing excessive strain on the joint.
- Response to Steroid Medication
Not everyone responds to corticosteroids in the same way. Some patients feel relief within a few days, while others may need more time. The duration of pain relief also varies, ranging from weeks to several months.
Your doctor may use your response to the injection to guide future treatment decisions. If the injection provides significant relief, it confirms the sacroiliac joint as the source of pain.
Tips for a Smooth and Faster Recovery
Supporting your body after the procedure can make a noticeable difference in how quickly you recover. Simple habits and precautions help reduce discomfort and improve outcomes.
Proper post-procedure care is not complicated, but consistency matters. Following your doctor’s instructions and listening to your body are the most effective ways to promote healing.
Small, consistent actions after the injection can significantly improve recovery speed and overall results.
Do’s and Don’ts After the Injection
Here are a few practical guidelines to follow:
- Rest during the first 24 hours after the procedure
- Apply ice to the injection site if soreness develops
- Avoid heavy lifting or intense exercise for several days
- Stay hydrated and maintain a balanced diet
- Gradually return to normal activities as pain allows
These steps help minimize irritation and support the healing process without overloading the joint.
When to Resume Normal Activities
Most patients can return to light activities within one to two days. Desk work and routine tasks are usually manageable shortly after the procedure. More physically demanding activities should be reintroduced slowly over the following week.
Exercise programs, especially those involving the lower back, should be resumed under guidance. Physical therapy may be recommended to strengthen supporting muscles and prevent recurrence of pain.
Warning Signs to Watch For
While complications are rare, it is important to be aware of potential warning signs. Severe pain, swelling, or redness at the injection site should not be ignored. Fever or unusual symptoms may indicate infection.
Persistent numbness or weakness beyond the first day also warrants medical attention. Prompt communication with your healthcare provider ensures any issues are addressed early.
How to Maximize Pain Relief After an SI Joint Injection
Getting the injection is only part of the process. What you do afterward plays a significant role in how effective the treatment will be. Patients who actively support their recovery often experience longer-lasting and more meaningful pain relief.
The goal is not just to reduce pain temporarily but to improve joint function and prevent future flare-ups. This involves a combination of movement, posture awareness, and healthy daily habits. Small adjustments can make a noticeable difference over time.
Maximizing the benefits of an SI joint injection depends largely on consistent post-procedure habits and lifestyle choices, often supported by personalized pain management plans tailored to your condition.
Strategies to Improve and Extend Pain Relief
- Follow a Guided Physical Therapy Plan
Strengthening the muscles around the pelvis and lower back helps stabilize the sacroiliac joint. A structured program can prevent recurring pain.
- Maintain Good Posture Throughout the Day
Sitting or standing incorrectly places unnecessary stress on the SI joint. Keeping your spine aligned reduces strain and supports healing.
- Use Heat or Ice Appropriately
Ice works best in the early days to reduce inflammation, while heat can help relax muscles later in recovery.
- Avoid High-Impact Activities Initially
Running, jumping, or heavy lifting can irritate the joint. Gradually reintroducing these activities prevents setbacks.
- Incorporate Low-Impact Exercise
Walking, swimming, and gentle stretching improve circulation and keep joints mobile without excessive stress.
- Manage Body Weight if Necessary
Extra weight increases pressure on the lower back and pelvis. Maintaining a healthy weight supports long-term joint health.
- Stay Consistent With Follow-Up Care
Attending follow-up appointments ensures your progress is monitored and adjustments are made if needed.
Why Lifestyle Changes Matter
Pain relief from the injection can last weeks or even months, but without supportive habits, symptoms may return. A 2021 report from the Centers for Disease Control and Prevention highlighted that lifestyle factors play a major role in managing chronic musculoskeletal pain.
This means recovery is not just about healing from the procedure but also about preventing future irritation. Patients who combine medical treatment with lifestyle improvements tend to see the best long-term outcomes.
By taking an active role in your recovery, you turn a short-term procedure into a more lasting solution for managing sacroiliac joint pain.
Comparing SI Joint Injection Recovery With Other Back Treatments
Understanding how this procedure compares to other treatments helps put recovery expectations into perspective. Sacroiliac joint injections are often chosen because they offer a balance of effectiveness and minimal downtime.
Unlike surgical options, injections do not require long recovery periods or hospitalization. Compared to physical therapy alone, they can provide faster relief, especially when inflammation is severe.
SI joint injections offer a shorter recovery time compared to many other back pain treatments, making them a practical first step.
| Treatment Type | Recovery Time | Invasiveness | Pain Relief Timeline |
| SI Joint Injection | Few days to 2 weeks | Minimally invasive | Days to weeks |
| Physical Therapy | Ongoing | Non-invasive | Gradual improvement |
| Spinal Surgery | Weeks to months | Highly invasive | Long-term recovery |
A 2021 study published by the National Institutes of Health found that minimally invasive treatments like joint injections often lead to quicker functional recovery compared to surgical interventions. This makes them a preferred option for many patients seeking relief without extended downtime.
Sacroiliac joint injection recovery time and What Comes Next
Understanding sacroiliac joint injection recovery time helps you approach treatment with realistic expectations and a clear plan. Most patients experience gradual improvement within the first week, with continued progress over the following weeks.
While the procedure itself is straightforward, recovery depends on how well you support your body afterward. For those who experience lasting relief, the next step often involves strengthening and maintaining joint stability through targeted exercises or physical therapy.
If pain returns, additional injections or alternative treatments may be considered. Exploring long-term strategies for managing lower back pain naturally leads into a broader conversation about prevention, posture, and lifestyle adjustments, as well as understanding long-term pain management strategies that support lasting relief..
Autoimmune diseases can be painful, but some stand out for the intensity and persistence of the discomfort they cause. The most painful autoimmune diseases are typically those that involve chronic inflammation, nerve damage, or widespread tissue involvement.
These conditions do more than create physical pain, as they reshape how a person moves, thinks, sleeps, and lives day to day. In many cases, the pain is ongoing and unpredictable, making it difficult to maintain a normal routine or plan ahead.
Understanding how they affect the body is the first step toward managing symptoms and improving quality of life in a meaningful, sustainable way. Let's look at the most painful autoimmune diseases and how they affect your body.
What Makes Some Autoimmune Diseases So Painful
Pain in autoimmune diseases is not random. It is the result of the immune system attacking healthy tissue, which leads to inflammation, swelling, and sometimes permanent damage.
This ongoing immune response creates a cycle where the body is constantly in a state of irritation, making pain both persistent and unpredictable.Inflammation plays a central role in this process.
When the immune system targets joints, muscles, or organs, it releases chemicals that increase blood flow and sensitivity in those areas. This leads to tenderness, stiffness, and a deep, aching sensation that can last for hours or even days.
Over time, repeated inflammation can wear down tissues and amplify pain signals. Nerve involvement adds another layer of discomfort. Some autoimmune conditions affect the nervous system directly, causing sharp, burning, or electric-like pain.
The combination of inflammation and nerve disruption is what makes certain autoimmune diseases especially difficult to manage. This is why people often describe their pain as both physical and deeply exhausting.
Key Factors That Intensify Autoimmune Pain
- Chronic inflammation that never fully resolves
- Damage to joints, muscles, or connective tissue
- Nerve involvement leading to sharp or burning sensations
- Flare ups triggered by stress, illness, or environmental factors
- Increased sensitivity to pain signals in the brain
Each of these factors contributes to how pain is experienced, and in many cases, several occur at the same time. This overlap is what makes autoimmune pain feel complex and difficult to predict.
Most Painful Autoimmune Diseases
Some autoimmune conditions are widely recognized for the level of pain they cause and the way that pain spreads throughout the body. While each disease has unique features, they share a common thread of chronic discomfort that can fluctuate in intensity.
Rheumatoid Arthritis
Rheumatoid arthritis targets the joints, especially in the hands, wrists, and knees. The immune system attacks the lining of the joints, causing swelling and stiffness that often feels worse in the morning.
Over time, the inflammation can lead to joint deformity and reduced mobility. The pain is usually symmetrical, meaning it affects both sides of the body in the same way.
This pattern can make everyday tasks like opening jars or walking long distances more difficult. Many people experience flare ups where the pain becomes more intense for a period of time.

Lupus
Lupus is known for its wide range of symptoms, including joint pain, muscle aches, and organ inflammation. It can affect the skin, kidneys, heart, and brain, making it one of the more complex autoimmune conditions.
The pain associated with lupus often shifts from one area of the body to another. Flare ups are common and can be triggered by stress, sunlight, or illness.
During these periods, pain may intensify and be accompanied by fatigue and fever. The unpredictability of lupus makes it especially challenging to manage on a daily basis.
Multiple Sclerosis
Multiple sclerosis affects the central nervous system, disrupting communication between the brain and the body. This can lead to nerve pain, muscle spasms, and a range of sensory issues. People often describe the pain as sharp, tingling, or burning.
Because the condition targets nerve pathways, symptoms can vary widely from person to person. Some may experience mild discomfort, while others face severe pain that interferes with movement and coordination.
The condition can also lead to long term disability if not managed carefully.
Fibromyalgia
Fibromyalgia is characterized by widespread musculoskeletal pain that affects multiple areas of the body. It is often accompanied by fatigue, sleep problems, and sensitivity to touch.
Unlike other autoimmune conditions, fibromyalgia does not cause visible inflammation, but the pain can be just as intense.
The condition is linked to how the brain processes pain signals. This means that even light pressure can feel overwhelming. Many people also experience brain fog, which makes it harder to concentrate or remember information.

Psoriatic Arthritis
Psoriatic arthritis combines joint pain with skin symptoms such as red, scaly patches. The condition often causes swelling in the fingers and toes, sometimes giving them a sausage-like appearance. Joint stiffness and fatigue are also common.
The pain can range from mild to severe and may worsen during flare ups. In some cases, it can lead to permanent joint damage if not treated early. The visible skin symptoms can also affect confidence and emotional well being.

How Chronic Pain Affects Daily Life
Living with chronic pain changes how a person approaches even the simplest tasks. Activities that were once routine, like getting dressed or preparing meals, can become physically demanding.
Over time, this can lead to frustration and a sense of loss of independence. Work and productivity are often affected as well. Many people with autoimmune diseases need to adjust their schedules or reduce their workload.
Some may require frequent breaks or accommodations to manage pain throughout the day. Emotional health is closely tied to physical well being. Chronic pain can lead to anxiety, depression, and feelings of isolation.
The constant presence of pain can make it difficult to stay engaged in social activities or maintain relationships. This creates a cycle where emotional stress further worsens physical symptoms.
Ways Chronic Pain Disrupts Everyday Life
- Reduced mobility, making basic movements slower and more difficult
- Decreased work capacity or the need for flexible schedules
- Interrupted sleep due to ongoing discomfort
- Difficulty maintaining social relationships and activities
- Increased emotional strain, including anxiety and depression
These disruptions often overlap, creating a ripple effect that impacts nearly every aspect of daily life. Recognizing these patterns can help individuals and caregivers take more proactive steps toward managing both physical and emotional challenges.
Common Symptoms Beyond Pain
Pain is only one part of the experience. Autoimmune diseases often come with a range of additional symptoms that can be just as disruptive.
These symptoms may appear gradually or suddenly, depending on the condition.Fatigue is one of the most common complaints.
It is not just feeling tired, but a deep exhaustion that does not improve with rest. This can make it difficult to maintain a regular routine or stay active throughout the day.
Cognitive issues, often referred to as brain fog, can affect memory, focus, and decision making. People may struggle to complete tasks or keep track of conversations. This can be especially challenging in professional settings.
Sleep disturbances are also common. Pain can make it hard to fall asleep or stay asleep, leading to a cycle of fatigue and worsening symptoms. Other complications may include skin changes, digestive issues, or organ involvement depending on the specific condition.
Diagnosis and Challenges in Identifying These Conditions
Diagnosing autoimmune diseases can be a long and complicated process. Many conditions share similar symptoms, which can make it difficult to pinpoint the exact cause. Patients often see multiple doctors before receiving a clear diagnosis.
Medical tests play an important role, but they are not always definitive. Blood tests, imaging, and physical exams are typically used together to identify patterns and rule out other conditions. Even with these tools, some diseases take years to confirm.
Early diagnosis is important because it allows for timely treatment. Without proper care, symptoms can worsen and lead to long term complications. Recognizing patterns in symptoms and seeking medical advice early can make a significant difference in outcomes.
Treatment Options for Managing Pain
Managing autoimmune pain requires a combination of medical treatment and lifestyle adjustments. There is no one size fits all approach, so treatment plans are often tailored to the individual.
Medications
Doctors may prescribe anti inflammatory drugs to reduce swelling and discomfort. Immunosuppressants are also commonly used to slow down the immune response.
In some cases, pain specific medications are added to address nerve related symptoms.These treatments can be effective, but they may come with side effects.
Regular monitoring is important to ensure that the benefits outweigh the risks.
Lifestyle Adjustments
Daily habits can have a strong impact on symptom management. A balanced diet that includes anti-inflammatory foods can help support overall health.
Regular physical activity, even in small amounts, can improve flexibility and reduce stiffness. Stress management is another key factor.
Techniques such as meditation, deep breathing, or gentle yoga can help reduce flare ups. Consistency in these habits often leads to better long term results.
Alternative Approaches
Some people find relief through complementary therapies. Acupuncture, massage, and physical therapy can help reduce pain and improve mobility. Support groups also provide a space to share experiences and learn coping strategies from others.
Living With Autoimmune Pain: Practical Coping Strategies
Adjusting to life with chronic pain takes time and patience. Building a routine that balances activity and rest can help prevent overexertion. Tracking symptoms can also provide insight into triggers and patterns.
Support systems play an important role. Family, friends, and healthcare providers can offer both practical and emotional support. Open communication about needs and limitations can make daily life more manageable.
Small, consistent changes often lead to meaningful improvements in how pain is experienced and managed. Over time, these strategies can help create a sense of stability and control.
- Stay consistent with treatment plans
- Prioritize rest and recovery
- Communicate openly with healthcare providers
- Seek emotional and mental health support
When to Seek Medical Help
Knowing when to seek medical attention is essential for managing autoimmune diseases. Sudden changes in symptoms, such as increased pain or new areas of discomfort, should not be ignored. These may indicate a flare up or progression of the condition.
Other warning signs include persistent fatigue, unexplained weight changes, or difficulty performing daily tasks. Early intervention can help prevent complications and improve quality of life.
Regular checkups are also important, even when symptoms are stable. This allows healthcare providers to monitor progress and adjust treatment plans as needed.
Most Painful Autoimmune Diseases
Understanding how these conditions affect the body highlights the importance of early care and consistent management. The most painful autoimmune diseases are not defined only by physical discomfort, but by how deeply they influence daily life, from movement to mental health.
Recognizing symptoms and seeking timely treatment can make a meaningful difference in long term outcomes. Looking ahead, exploring how to reduce flare ups and improve long term wellness offers a natural next step for anyone navigating life with autoimmune conditions.
No, osteoporosis does not directly cause pain if there are no fractures. Osteoporosis is fundamentally a metabolic skeletal disorder defined by reduced bone strength and an increased risk of fracture.
The condition develops from an imbalance between bone resorption and bone formation, leading to deterioration of the bone’s internal structure. Many people assume this weakening causes a constant dull ache or deep soreness in the bones.
In reality, bone tissue lacks the dense network of pain fibers found in surrounding structures, so this gradual breakdown does not directly trigger pain signals. The key clinical distinction is between pain caused by an actual fracture and discomfort that arises later from mechanical dysfunction in a weakened skeleton. Does osteoporosis cause pain if there are no fractures? Let's find out.
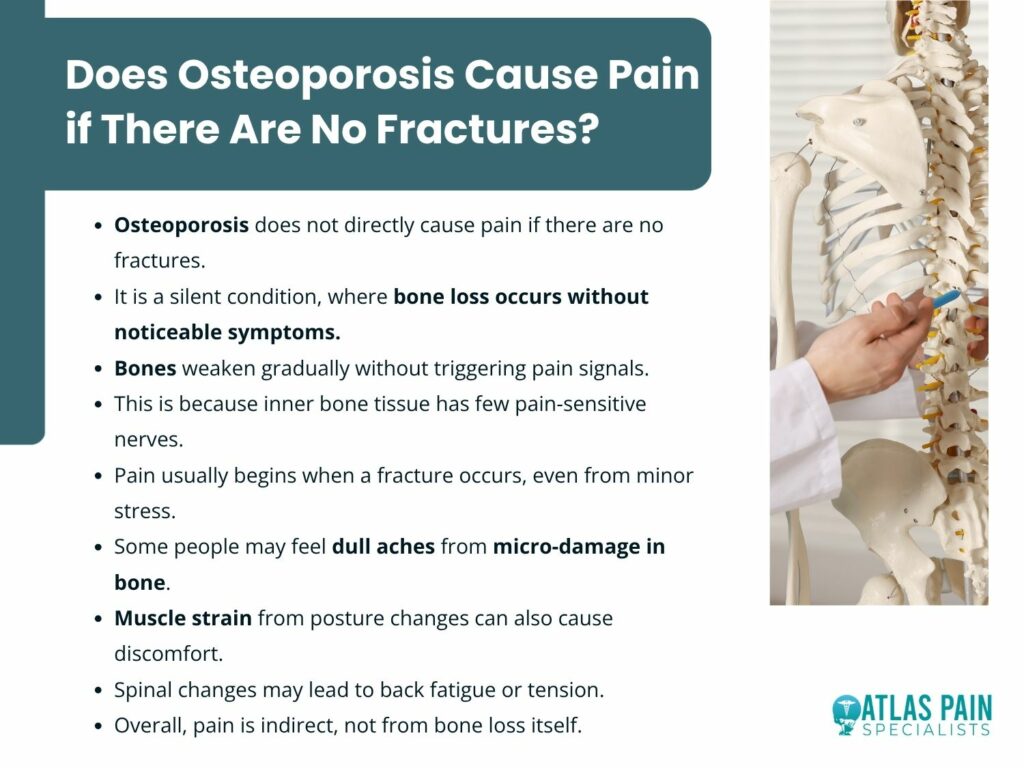
The Asymptomatic Nature of Bone Loss in Osteoporosis
Osteoporosis is often described as a silent disease, but this description reflects a specific anatomical and physiological reality rather than a general absence of pathology. The processes that weaken bone structure occur largely without activating the body’s pain detection systems, allowing significant deterioration to develop before any symptoms appear.
The Absence of Sensory Innervation Within Bone
Bone is a living tissue, but its internal structure lacks the components needed to transmit pain signals to the central nervous system. Nociceptors, which detect mechanical, thermal, or chemical damage, are located mainly in the periosteum, the dense outer membrane of the bone.
The trabecular interior and cortical bone contain very few of these nerve endings. As a result, gradual demineralization does not activate pain receptors.
Osteoclasts resorb bone and osteoblasts form new matrices without stimulating surface nerves. This separation explains why bone turnover remains a silent process even when resorption exceeds formation.
The Painless Nature of Microarchitectural Deterioration
The disease process involves a reduction in the connectivity of the trabecular plates and rods within the cancellous bone. This structural decay weakens the internal support system, but it does not produce a sensation of pain.
The collapse of these individual struts happens below the threshold of human perception.
- The loss of bone mineral density occurs gradually over years, allowing the body to adapt without sending distress signals.
- The microfractures that occur at the cellular level are too small to disturb the periosteum, which remains intact and unstimulated.
- There is no inflammatory component associated with simple bone thinning, unlike arthritis which involves swollen and irritated joint linings that press against sensitive tissues.
The Periosteum as the Threshold for Sensation
The periosteum serves as the critical boundary between silent pathology and conscious pain. This membrane contains a rich network of sensory nerves that respond to stretching, tearing, or impact.
In the absence of a fracture that disrupts this outer layer, the weakened bone underneath can continue to deteriorate without ever engaging these sensitive nerve fibers. For a patient to feel direct bone pain, the structural failure must extend to the surface where the nerves reside.
A non-displaced vertebral fracture or a crack in the cortical bone will stretch the periosteum and generate a sharp, localized signal. Until that mechanical event occurs, the disease remains hidden from the patient's sensory awareness.
The Pain That Comes From Posture Changes
As osteoporosis progresses, structural changes within the spine can lead to significant alterations in posture. These changes do not directly cause bone pain but instead create secondary mechanical strain on muscles, ligaments, and joints, resulting in persistent discomfort and functional limitations.
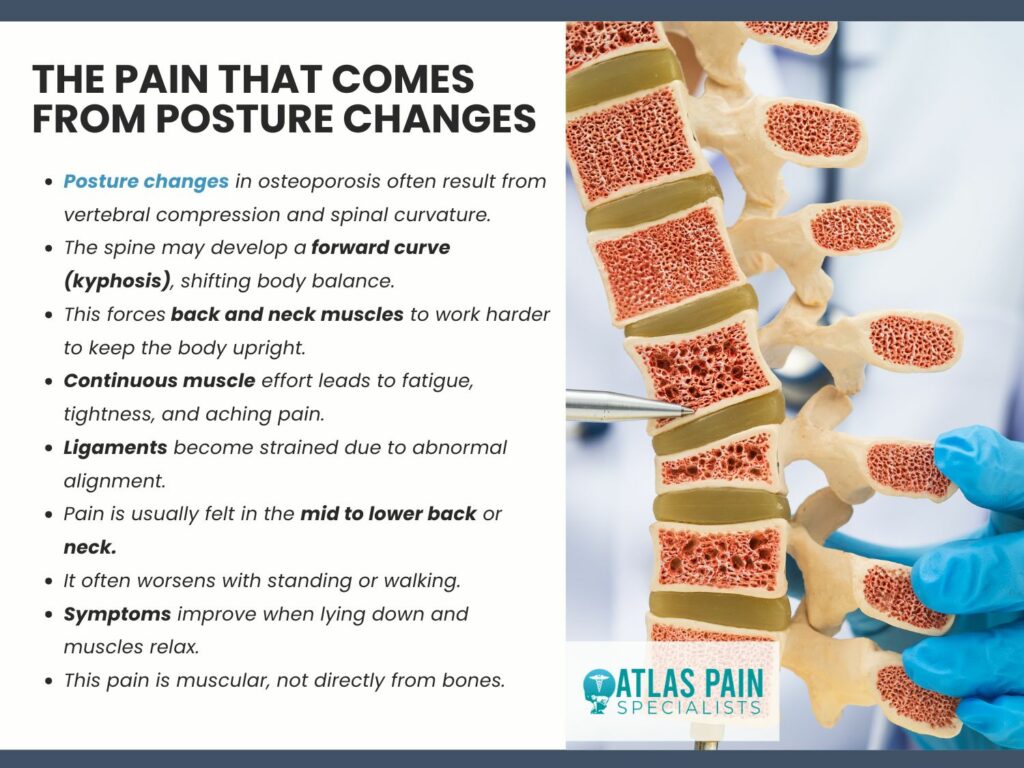
- The Biomechanical Shift of Vertebral Collapse
The thoracic spine supports the weight of the upper body and maintains the upright position against gravity. When multiple vertebral bodies lose height due to compression fractures, even those that go undiagnosed, the natural alignment of the spinal column shifts forward.
This creates an increased thoracic kyphosis, a curvature that forces the head and neck to extend backward to maintain a horizontal gaze. This realignment places the center of mass anterior to the pelvis.
The body compensates by recruiting posterior chain muscles to prevent a forward fall. The paraspinal muscles, erector spinae, and deep stabilizers must work continuously to counteract this force, leading to fatigue and localized tenderness.
- Compensatory Muscle Strain and Ligamentous Stress
The soft tissues surrounding the spine were not designed to bear the load created by a severely curved posture. Ligaments along the anterior portion of the spine become slack while those in the posterior are placed under constant tension
- The cervical extensors contract forcefully to keep the head level, which often results in tension headaches and upper neck pain.
- The lumbar erector spinae work excessively to stabilize the lower back, as the thoracic curve above disrupts the efficient transfer of load through the vertebral column.
The costovertebral joints, where the ribs attach to the spine, can become irritated from the altered thoracic shape, producing a dull ache near the shoulder blades that mimics lung or cardiac referral patterns.
- Pain Originating From Overworked Muscles
The sensation experienced by many individuals with advanced osteoporosis is not bone pain but myofascial pain from constantly contracted muscles. These muscles accumulate metabolic waste and develop trigger points due to the ongoing effort required to maintain posture.
Patients often describe a burning sensation along the spine or a deep ache in the lower back that worsens throughout the day. This pain follows the pattern of overworked muscles rather than a specific dermatome.
The discomfort improves with lying down, which reduces gravitational load and allows the muscles to relax. It returns upon standing as the muscles resume compensating for the altered spinal alignment.
The Difference Between a Fracture and a Micro-Fracture
Bone damage presents in different forms, and understanding the difference between a full fracture and a micro-fracture is critical for interpreting symptoms. Both involve structural compromise, but they differ significantly in severity, visibility on imaging, and the type of pain they produce.
This distinction becomes especially important in conditions like osteoporosis, where bone weakening occurs gradually.
- The Clinical Fracture Event
A clinical fracture represents a complete or partial break in the bone that is visible on standard radiographs. It involves disruption of the cortical bone and often includes displacement of bone fragments.
The mechanical failure is severe enough to stretch or tear the periosteum, which contains a dense network of pain fibers. This produces a sharp and localized pain signal.
Pain from a fracture is acute and closely linked to movement. Weight bearing becomes difficult or impossible, and surrounding muscles tighten to limit motion while the pain gradually improves as healing occurs.
- The Nature of Micro-Fractures in Weakened Trabeculae
Micro-fractures, sometimes called microfissures or stress reactions, occur within individual trabeculae in the cancellous bone. These tiny cracks do not extend through the full thickness of the bone or disrupt the outer cortical surface.
In healthy bone, these micro-fractures heal through normal remodeling without producing symptoms. In osteoporotic bone, the rate of accumulation exceeds the capacity for repair.
The trabecular network becomes weakened and inefficient at transmitting forces. These small failures create localized bone edema and mild inflammation within the marrow, which can generate a low-level pain signal.
- Differentiating Pain Quality and Presentation
The sensory experience of a micro-fracture differs substantially from that of a complete fracture. Patients do not report a sudden, sharp pain associated with a specific incident.
Instead, they describe a diffuse, dull ache located deep within a region, such as the hip or the low back, that appears during sustained weight bearing and fades with rest.
- The pain tends to be activity-dependent rather than constant, appearing after walking for a certain distance or standing for prolonged periods.
- There is no single point of tenderness that the patient can identify with a finger, as the discomfort arises from a region of accumulated micro-damage rather than a single disrupted site.
Percussion over the bone may reproduce a mild ache, but it does not elicit the sharp wincing response seen with a true fracture.
How Spinal Changes Cause Abdominal Discomfort
Advanced osteoporosis affects more than bone strength alone; it alters the structural relationships within the torso. As vertebral compression fractures change the shape of the spine, they reduce space in the chest and abdomen, placing pressure on internal organs and causing digestive and breathing symptoms.
The Anatomical Consequences of Thoracic Kyphosis
The thoracic spine forms the posterior wall of the chest cavity and provides the attachment points for the ribs. When multiple vertebral compression fractures occur in the mid to lower thoracic region, the spinal column shortens and curves forward.
This collapse reduces the vertical dimension of the thorax, forcing the rib cage downward toward the iliac crests of the pelvis. The space available for the abdominal viscera becomes constrained.
The stomach, the transverse colon, and the small intestine normally occupy a volume that depends on adequate separation between the diaphragm and the pelvic floor. As the rib cage descends, it compresses the abdominal contents against the pelvic basin, leaving less room for distention after meals and less space for normal peristaltic movement.
Gastrointestinal Symptoms From Mechanical Compression
Patients with significant height loss from osteoporosis frequently report a cluster of digestive complaints that have no primary gastrointestinal pathology. These symptoms arise purely from the altered geometry of the trunk and the resulting pressure on hollow organs.
- Early satiety occurs because the stomach cannot expand fully when compressed between the diaphragm and the anterior abdominal wall, leading to a sensation of fullness after only small amounts of food.
- Gastric reflux increases as the intra-abdominal pressure rises, pushing gastric contents against a lower esophageal sphincter that now sits at a different angle relative to the stomach.
- Constipation develops from mechanical slowing of colonic transit, as the descending colon must navigate a shortened and crowded abdominal cavity.
- Bloating and abdominal distention appear after meals as swallowed air and digestive gases have limited space to disperse.
The Sensation of Pain Referred to the Abdomen
The discomfort associated with these mechanical changes does not originate from the spine itself but from the viscera under pressure. Patients often describe a vague, pressure-like ache in the upper abdomen or around the flanks that they cannot localize precisely.
This sensation differs from the sharp, movement-related pain of a vertebral fracture. The phrenic nerve and the lower intercostal nerves innervate both the diaphragm and the peritoneum.
When the descending rib cage irritates these structures, the brain can misinterpret the signal as originating from the upper abdominal organs. This referred pattern leads some patients to undergo evaluations for gallbladder disease or peptic ulcers when the true cause is the postural collapse of their osteoporotic spine.
Back Hurts When I Sneeze: Is It Normal or a Sign of Something More?
Osteoporosis remains a silent condition until the skeleton reaches a point where it can no longer handle normal mechanical stress without damage. The symptoms people feel are not caused by bone loss itself but by the effects that follow, including structural changes and fractures.
A sudden sharp pain in the back during a sneeze clearly demonstrates this. The force created by the movement, along with muscle contraction, is normally well tolerated by a healthy spine.
When that same force causes immediate localized pain in someone with osteoporosis, it suggests that the vertebra has likely failed. What seems like a simple reflex becomes an important sign that requires medical evaluation.
Back and nerve pain affect millions of adults across the United States every year, often interfering with everyday activities such as walking, driving, or sitting comfortably at work.When conservative treatments like physical therapy, medications, or lifestyle changes do not provide enough relief, physicians may recommend an epidural steroid injection to reduce inflammation around irritated spinal nerves.
Because the procedure is minimally invasive, many patients expect a quick recovery but still wonder how much rest is necessary afterward. How long should you rest after an epidural steroid injection? In most cases, doctors recommend limiting activity for about 24 hours before gradually returning to normal routines.
Understanding the recovery timeline helps patients protect the injection site while giving the medication time to reduce inflammation and improve mobility.
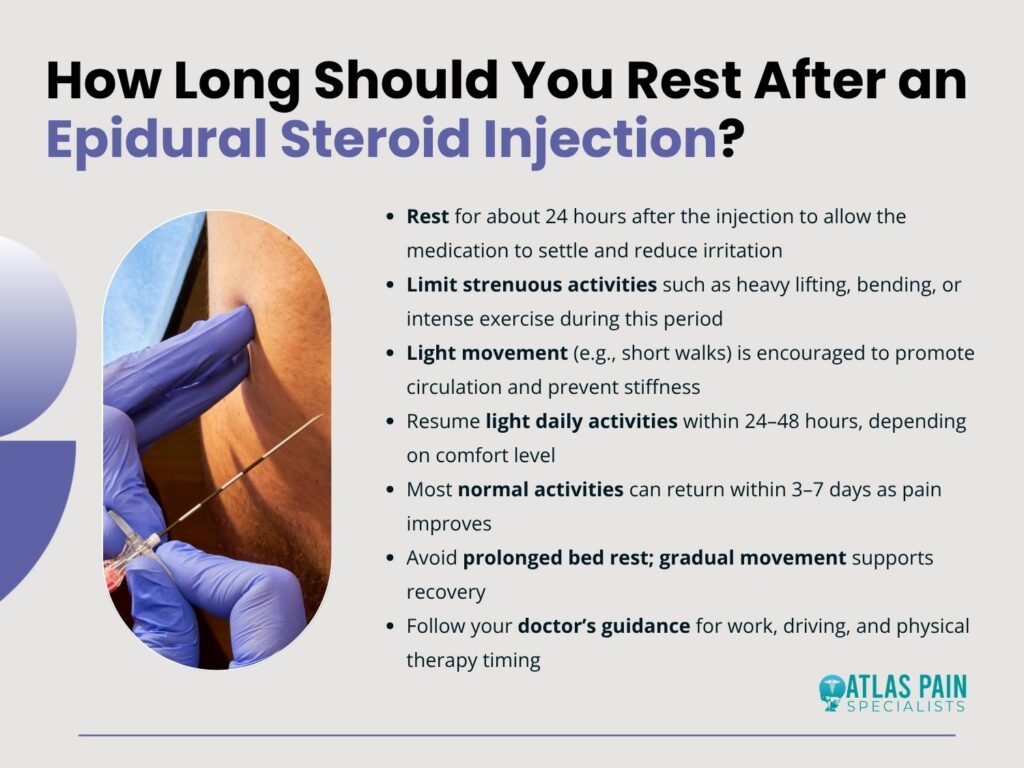
Understanding Epidural Steroid Injections and Their Purpose
An epidural steroid injection is a common non surgical treatment used to manage nerve related spinal pain. During the procedure, a physician injects corticosteroid medication into the epidural space around the spinal cord and nerve roots.
The goal is to reduce inflammation and swelling around irritated nerves, which can relieve pain and improve mobility. Epidural steroid injections target inflammation at its source, helping calm irritated nerves and allowing patients to move more comfortably.
What Happens During the Procedure
The procedure usually takes place in an outpatient clinic or hospital setting and typically lasts less than 30 minutes. Doctors use imaging technology such as fluoroscopy to guide a thin needle into the epidural space with precision.
Once the needle is positioned correctly, a mixture of corticosteroid medication and a local anesthetic is injected.The anesthetic provides immediate but temporary pain relief, while the steroid medication works gradually over several days to reduce inflammation.
Patients are typically monitored for a short time after the procedure and are then able to return home the same day. Because the treatment does not involve surgery, the recovery period is usually short.
Conditions Commonly Treated
Physicians use epidural steroid injections to treat several spinal conditions that cause nerve irritation and inflammation. These include herniated discs, spinal stenosis, degenerative disc disease, and sciatica.
Each of these conditions can place pressure on spinal nerves, leading to pain that radiates into the arms or legs. According to the American Society of Interventional Pain Physicians in its 2021 clinical guidelines, epidural steroid injections remain one of the most widely used non surgical treatments for spinal nerve pain in the United States.
By reducing inflammation around nerve roots, these injections can provide meaningful relief and allow patients to participate more actively in rehabilitation or physical therapy programs.
Who Is a Good Candidate for Epidural Steroid Injections
Not every patient with back pain needs this type of treatment. Doctors usually recommend epidural steroid injections for individuals experiencing nerve related pain that has not improved with other therapies.
These injections are typically considered when inflammation around spinal nerves is clearly identified and other conservative treatments have not produced enough relief. Patients who meet specific medical criteria are more likely to benefit from epidural steroid injections as part of a broader pain management plan.
Many physicians evaluate candidates based on symptoms, diagnostic imaging, and response to previous treatments. In general, patients who may benefit from the procedure include:
- Individuals with nerve pain caused by herniated discs or spinal stenosis
- Patients who have tried physical therapy or medications without sufficient improvement
- People experiencing radiating pain such as sciatica that travels into the legs or arms
- Patients looking to delay or avoid spinal surgery
- Individuals who need temporary pain relief to participate in rehabilitation programs
Imaging tests such as MRI or CT scans are often used to confirm nerve compression before the procedure is recommended. According to the American Academy of Orthopaedic Surgeons in 2022, epidural injections are frequently used when conservative treatments fail to control nerve inflammation but surgery is not immediately necessary.
For many patients, the injection provides a window of reduced pain that allows them to participate more fully in physical therapy and strengthen the muscles supporting the spine.
Recommended Rest Time After an Epidural Steroid Injection
After receiving the injection, a short period of rest helps the body adjust to the medication and protects the treated area from irritation. Although the procedure is minimally invasive, the tissues surrounding the spine may still be sensitive during the first day.
Doctors usually recommend limiting strenuous activity during this initial recovery period. For most patients, about 24 hours of reduced activity is enough before gradually returning to normal movement.
The First 24 Hours
The first day after the injection is mainly focused on rest and gentle movement. Patients are typically advised to relax at home for the remainder of the day after the procedure.
Short walks around the house are usually encouraged because they promote circulation and help prevent stiffness.Strenuous activities such as lifting heavy objects, bending repeatedly, or intense exercise should be avoided during this time.
Some patients may notice mild soreness at the injection site or temporary numbness caused by the anesthetic. These symptoms usually fade within a day or two.
Typical Recovery Timeline
Recovery can vary depending on the patient’s health and the condition being treated, but physicians often describe the process in stages as the medication begins working.
| Time After Injection | Recommended Activity | What Patients May Feel |
| First 24 hours | Rest and light walking | Mild soreness or numbness |
| 24 to 48 hours | Resume light daily activities | Gradual pain improvement |
| 3 to 7 days | Return to most normal activities | Steroid begins full effect |
| 1 to 2 weeks | Physical therapy may begin | Increased mobility |
According to the American Academy of Orthopaedic Surgeons in 2022, steroid medications often require several days to fully reduce inflammation around irritated nerves. As swelling decreases, many patients experience improved movement and reduced pain.
Why Gradual Movement Helps Recovery
While rest is important during the first day, complete bed rest for several days is usually not recommended. Gentle movement helps maintain circulation, which supports the body’s natural healing process.
Walking short distances and performing light daily tasks can also prevent stiffness in the muscles surrounding the spine. A 2021 guideline from the North American Spine Society explains that light movement following spinal procedures often improves recovery and reduces discomfort caused by prolonged inactivity.
Gradually increasing activity levels allows the body to adjust to the steroid medication while protecting the treated area from excessive strain.Patients are often encouraged to listen to their bodies and slowly reintroduce regular activities as symptoms improve.
Activities to Avoid During the Initial Recovery Period
Although most patients recover quickly after the procedure, avoiding certain movements during the early recovery phase helps protect the injection site. Excessive strain on the spine can irritate the treated area and delay the anti-inflammatory effects of the medication.
Taking a cautious approach to physical activity during the first few days helps ensure the injection delivers its intended benefits.
Physical Activities to Limit
Doctors typically advise patients to avoid several types of activity that place unnecessary pressure on the spine:
- Heavy lifting or carrying large objects
- Intense exercise or gym workouts
- Twisting or bending movements that strain the back
- High impact sports such as running or jumping
- Long periods of sitting without standing or stretching
These restrictions are usually temporary and last only a few days. Once soreness decreases and mobility improves, patients can gradually resume their normal physical routines.
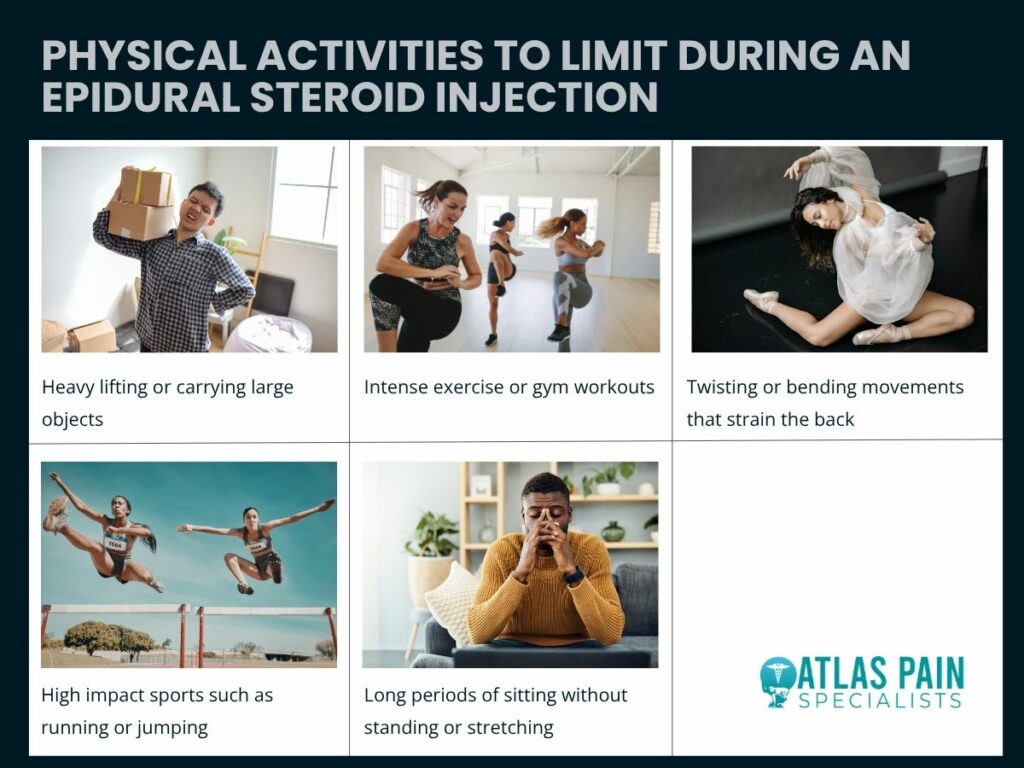
Driving and Work Considerations
Driving immediately after the injection may not be recommended, especially if sedation was used during the procedure. Patients are often advised to arrange transportation home and wait until any numbness or weakness from the anesthetic has completely worn off.
Returning to work depends largely on the type of job a patient has. Individuals with desk based roles may return the following day, while those with physically demanding jobs may need additional time before resuming full duties.
According to the Cleveland Clinic in 2023, most people can return to regular daily activities within one or two days after an epidural injection, although strenuous physical work may require additional recovery time.
Tips for a Comfortable Recovery at Home
Simple habits at home can make the recovery period easier and more comfortable. Many physicians recommend applying an ice pack to the injection site if mild soreness develops. Ice can help reduce inflammation and relieve discomfort during the first day or two.
Maintaining good posture while sitting and sleeping can also support spinal recovery. Using a supportive chair or placing a small pillow behind the lower back can reduce pressure on the spine. Gentle walking throughout the day helps prevent stiffness and keeps muscles active.
According to the Cleveland Clinic in 2023, applying ice and maintaining light movement can significantly reduce post injection soreness and improve overall comfort during recovery.
Signs of Normal Recovery and When to Contact a Doctor
Most patients experience mild and temporary sensations after an epidural steroid injection as the body adjusts to the medication. These symptoms are generally part of the normal healing process and often resolve quickly.
Understanding what typical recovery feels like helps patients avoid unnecessary worry while monitoring for unusual symptoms.
Normal Side Effects
The most common side effect is mild soreness near the injection site. This discomfort often feels similar to a small bruise and typically fades within a day or two.
Some patients may also experience temporary numbness or weakness due to the anesthetic included in the injection.Pain relief sometimes occurs in stages.
The anesthetic may provide immediate relief that fades after several hours, followed by the gradual anti-inflammatory effect of the steroid medication. According to the Cleveland Clinic in 2023, many patients begin noticing improvement in symptoms within three to seven days after the injection.
Warning Signs That Need Medical Attention
Although complications are rare, certain symptoms should be evaluated by a healthcare professional. Severe headaches that worsen when standing, fever, swelling near the injection site, or persistent numbness should be discussed with a physician.
Patients should also contact their doctor if pain significantly worsens or if unusual neurological symptoms appear. Prompt evaluation helps ensure that any rare complications are addressed quickly and safely.
How Long Should You Rest After an Epidural Steroid Injection
Recovery after this procedure is typically quick compared with many other treatments for spinal pain. For most people, resting for about 24 hours and gradually resuming normal activity provides enough time for the body to adjust to the medication.
Light movement during the following days often supports healing by improving circulation and preventing stiffness.Many physicians recommend combining epidural injections with physical therapy, stretching, and strengthening exercises once inflammation decreases.
According to the American Society of Interventional Pain Physicians in 2021, epidural steroid injections are often most effective when used as part of a broader pain management strategy.While some patients experience relief lasting several months, others may require repeat injections depending on the severity of their condition.
Understanding the recovery timeline helps patients approach the procedure with confidence while preparing for the next steps in long term spine health and pain management.
Shoulder pain can make simple daily tasks difficult, which is why cortisone injections are commonly used to reduce inflammation and restore movement. Many patients who receive this treatment ask a practical question before leaving the clinic: can they safely drive themselves home afterward.
In most cases, people are able to drive after a shoulder injection, but the answer depends on factors such as temporary numbness from anesthetic medication, pain levels, and which arm was treated. Can you drive after a cortisone injection in the shoulder? Understanding what happens immediately after the procedure can help patients plan transportation and avoid unnecessary strain while the shoulder begins to recover.
Understanding How Cortisone Injections Work in the Shoulder
Cortisone injections are frequently used to treat inflammation within the shoulder joint or surrounding tissues. These injections contain corticosteroids, a type of medication designed to reduce swelling and irritation in areas where tendons, ligaments, or bursae become inflamed.
When inflammation decreases, many patients experience noticeable relief from pain and improved mobility in the joint.Doctors often recommend this treatment when rest, physical therapy, or oral medications have not fully resolved shoulder discomfort.
The injection is typically delivered directly into the affected joint or nearby bursa using a thin needle. This targeted approach allows the medication to work precisely where inflammation is occurring.
A 2021 clinical overview from the American Academy of Orthopaedic Surgeons explained that corticosteroid injections are widely used to reduce inflammation in joints affected by injury, arthritis, or overuse conditions.
Because the shoulder joint is highly mobile and vulnerable to strain, injections are often part of a broader plan to restore movement and reduce chronic discomfort.Cortisone injections help calm inflammation in the shoulder joint so that pain decreases and normal movement gradually becomes easier.
What Cortisone Does Inside the Joint
Corticosteroids mimic hormones naturally produced by the adrenal glands. When injected into an inflamed joint, the medication suppresses the immune response responsible for swelling and irritation.
This process allows irritated tissues around the shoulder to settle down and heal.Pain relief does not always happen immediately. Some patients feel improvement within a few days, while others notice gradual progress over the next one to two weeks.
The anti-inflammatory effects may last several weeks or even months depending on the underlying condition.
Common Shoulder Conditions Treated With Cortisone
Doctors often recommend shoulder injections for inflammatory conditions that restrict movement or cause persistent pain. These problems typically affect tendons, bursae, or the joint lining itself.
Common conditions treated with cortisone injections include:
- Rotator cuff tendinitis
- Shoulder bursitis
- Frozen shoulder
- Shoulder arthritis
- Shoulder impingement syndrome
In many cases, the injection works best when combined with rehabilitation exercises designed to strengthen the muscles that support the shoulder joint.
Can You Drive After Cortisone Injection in Shoulder?
The short answer is that many patients can drive after a cortisone injection, but doctors frequently recommend waiting until the effects of the local anesthetic wear off and the shoulder feels stable.
Immediately after the procedure, the injected area may be numb or slightly weak, especially if lidocaine or a similar anesthetic was used during the treatment.The anesthetic helps minimize discomfort during the injection itself, but it can temporarily affect sensation and muscle control in the shoulder or arm.
Because driving requires steering control and quick reactions, even mild numbness may reduce the ability to safely operate a vehicle. According to the Mayo Clinic in 2022, local anesthetic is commonly included in corticosteroid injections to provide short term pain relief during and shortly after the procedure.
While this improves comfort, it can temporarily alter sensation in the treated area.Most physicians advise patients to test their shoulder movement before getting behind the wheel.
If the arm feels heavy, numb, or weak, waiting several hours before driving is usually the safest choice.Waiting until the shoulder regains full sensation and strength helps ensure that steering and reaction time remain safe while driving.
Why Some Doctors Suggest Waiting Before Driving
Driving involves coordinated arm movement, especially when turning the steering wheel, adjusting mirrors, or reacting quickly to traffic conditions. Even a small reduction in shoulder strength or flexibility can affect control of the vehicle.
For this reason, some doctors recommend arranging a ride home after the injection. This precaution removes pressure from the shoulder while the anesthetic fades and allows the patient to rest during the initial recovery period.
If a patient does plan to drive, it is important to confirm that shoulder movement feels normal and that the arm can comfortably perform steering motions without pain or stiffness.
What to Expect Immediately After the Injection
The hours following a cortisone injection are usually uneventful for most patients. Many people leave the clinic feeling relatively comfortable, particularly because the anesthetic temporarily reduces pain around the injection site. However, the shoulder may feel slightly different during the first several hours.
Some individuals notice a sensation of heaviness or numbness in the arm. This occurs when the anesthetic spreads through nearby tissues and affects local nerves. The sensation typically fades within a few hours as the medication wears off.
Another possibility is a short term increase in discomfort known as a post injection flare. Although it may sound concerning, this reaction is generally mild and temporary. The American College of Rheumatology reported in 2020 that a small percentage of patients experience a brief increase in pain within the first day after a corticosteroid injection.
Temporary Numbness or Weakness
Because the shoulder joint connects to several nerves that control arm movement, anesthetic medication may temporarily affect muscle control in the surrounding area. The arm might feel slightly weak or difficult to lift fully for a short period.
This effect usually fades within three to six hours. Once sensation and strength return, most people can resume normal daily activities with minimal limitations.
Possible Post Injection Flare
A post injection flare occurs when the joint becomes irritated for a short time after the medication enters the area. This reaction may cause mild swelling or soreness, but it typically resolves within one or two days.
Common short term symptoms may include:
- Mild soreness at the injection site
- Temporary numbness in the shoulder or arm
- Warmth or flushing in the treated area
- Slight swelling near the joint
- A brief increase in discomfort before relief begins
Applying an ice pack and limiting strenuous shoulder activity can help ease these symptoms while the joint settles.
Most temporary side effects after a cortisone injection resolve quickly and are considered a normal part of the recovery process.
Factors That Determine When It Is Safe to Drive
Every patient responds slightly differently to shoulder injections, which is why doctors often give individualized advice about driving afterward. Several factors influence whether a person can safely operate a vehicle soon after the procedure.
One important consideration is which arm received the injection. The dominant arm often performs more steering and control movements, so temporary weakness in that arm may make driving more difficult. Pain levels and shoulder mobility also play a role in determining readiness to drive.
Testing shoulder movement before leaving the parking lot can help determine whether driving feels comfortable. If turning the steering wheel causes discomfort or stiffness, waiting longer before driving is the safest option.
| Factor | Why It Matters | Typical Recommendation |
| Which arm received the injection | Steering requires coordinated arm movement | Non dominant arm may allow earlier driving |
| Use of anesthetic | Numbness can reduce control | Wait until full sensation returns |
| Pain level | Discomfort may limit movement | Drive only if shoulder feels comfortable |
| Range of motion | Limited movement affects steering | Test movement before driving |
| Doctor instructions | Individual medical advice varies | Follow provider guidance |
Some patients also receive ultrasound guided injections, which allow doctors to place medication precisely in the affected area. This technique may reduce discomfort afterward, but it does not necessarily change driving recommendations.
Safe driving after a shoulder injection depends on having full shoulder control, normal sensation, and the ability to move the arm without pain.
Tips for a Safe Recovery After a Shoulder Cortisone Injection
The first day after a cortisone injection is primarily focused on allowing the medication to settle into the joint. While most people can return to light activities quickly, doctors often recommend limiting strenuous shoulder movement during the first twenty four hours.
This brief recovery period gives the joint time to respond to the medication and helps prevent unnecessary irritation around the injection site. Even though cortisone reduces inflammation, the joint may still be sensitive immediately after the procedure.
Arrange Transportation When Possible
Bringing a friend or family member to the appointment can remove uncertainty about driving home. If numbness or soreness occurs after the injection, having someone else handle transportation allows the patient to rest without worrying about shoulder movement.
This precaution is particularly helpful when the injection is given in the dominant arm.
Limit Shoulder Activity for the First Day
Doctors often recommend avoiding heavy lifting or repetitive shoulder movement during the first day after treatment. Gentle movements such as walking or light daily activities are usually fine, but strenuous exercise should be postponed until the shoulder feels stable.
Once the initial soreness fades, many patients begin stretching or physical therapy exercises designed to restore shoulder strength.
Monitor Symptoms
Although complications are uncommon, patients should monitor the injection site for unusual symptoms. Persistent swelling, severe pain, or signs of infection should be reported to a healthcare provider.
The National Health Service noted in its 2022 patient guidance that most individuals return to normal daily activities within a day or two after receiving a corticosteroid injection. This quick recovery is one reason the treatment remains widely used for joint inflammation.
Allowing the shoulder to rest briefly after the injection supports healing and helps the medication work effectively.
Can You Drive After Cortisone Injection in Shoulder
Driving after a shoulder cortisone injection is often possible later the same day, but the decision should be based on comfort, mobility, and sensation in the treated arm. Temporary numbness from anesthetic medication may affect strength or coordination for a few hours, which is why some doctors recommend arranging transportation or waiting before driving.
Once the shoulder regains normal movement and the arm feels steady, many patients can safely resume routine activities including driving. Understanding how the injection works and what to expect during recovery helps patients make informed decisions after treatment.
Exploring how cortisone injections fit into long term shoulder pain management also opens the door to discussions about rehabilitation exercises and preventive strategies.