The decision to receive an epidural injection, whether for labor analgesia or surgical anesthesia, requires a clear understanding of the preparatory steps involved. The medications and substances present in your body directly influence the safety and efficacy of the procedure.
Anesthesiologists must have a complete picture of your recent intake to mitigate risks such as bleeding complications or adverse drug interactions. Patient cooperation with pre-procedural guidelines is a critical component of anesthetic safety.
What not to take before an epidural injection? Certain common foods, supplements, and medications can directly counteract the body's natural clotting mechanisms or alter its response to emergency medications. Failure to observe these restrictions may result in the postponement of the procedure for medical reasons.
1. Blood Thinning Medications and Supplements
An epidural injection requires precise placement into a space housing delicate blood vessels. The needle or catheter can inadvertently puncture one of these vessels during the procedure. A substance that inhibits the blood's ability to clot increases the risk of a significant bleed in this confined area.
Such an event, though rare, can lead to compression of spinal nerves and requires immediate medical intervention. The anesthesiologist must have a complete and accurate list of everything the patient has ingested in the days prior.
Prescription Anticoagulants
Patients prescribed medications to prevent thrombosis or manage cardiac conditions must follow specific timing protocols. These drugs are designed specifically to alter the clotting cascade and cannot be combined safely with an epidural.
- Warfarin (Coumadin): This medication requires several days for the effects to diminish after the last dose.
- Clopidogrel (Plavix): This antiplatelet drug impairs platelet function for the lifespan of the platelet itself.
- Enoxaparin (Lovenox): This injectable anticoagulant has a shorter duration of action but still requires precise timing.

Over-the-Counter Pain Relievers
Non-prescription pain medications are common household items that many people take without a second thought. These drugs can have profound effects on platelet activity and bleeding time.
- Aspirin: This drug permanently inhibits platelet function for the cell's entire lifespan.
- Ibuprofen (Advil, Motrin): These nonsteroidal anti-inflammatory drugs (NSAIDs) interfere with platelet function temporarily.
- Naproxen (Aleve): This longer-acting NSAID remains in the system for an extended period compared to ibuprofen and requires careful consideration regarding the timing of the last dose.
Herbal Supplements and Natural Products
The herbal supplement market is not regulated with the same rigor as pharmaceutical drugs regarding purity and potency. Many of these products contain active compounds that directly affect coagulation or platelet aggregation.
- Garlic: High doses of garlic can inhibit platelet aggregation and prolong bleeding time. Its effect can be significant enough to be problematic in combination with other factors.
- Ginkgo Biloba: This supplement is known to inhibit platelet-activating factor. Several case reports have linked ginkgo use to spontaneous bleeding events.
- Fish Oil (Omega-3 Fatty Acids): High doses of fish oil can reduce platelet aggregation. Patients are often advised to discontinue these supplements a few days before the procedure.
- Ginseng: This herb can affect both clotting time and the efficacy of other anticoagulant medications the patient may be taking.
The standard recommendation involves discontinuing these products for a period of one to two weeks prior to the scheduled epidural to ensure complete clearance from the system.
2. Heavy Meals and Large Amounts of Food
The presence of solid food in the stomach during an epidural placement presents a specific physiological danger. An epidural is most often used for procedures where the patient remains awake, but the clinical situation can change without warning.
Anesthesiologists manage the airway with the assumption that the stomach may contain food particles. These solid particles can migrate from the stomach into the lungs if protective reflexes are lost.
The resulting chemical injury to the lung tissue, known as aspiration pneumonitis, carries significant morbidity. The fasting period exists specifically to reduce the volume and acidity of stomach contents.
Specific Fasting Guidelines
The American Society of Anesthesiologists provides standardized fasting recommendations for elective procedures. These guidelines apply to patients of all ages undergoing anesthesia or sedation.
The times listed represent minimum intervals and may be extended based on individual patient factors or facility policies.
| Ingested Material | Minimum Fasting Period |
| Clear liquids (water, clear juice, black coffee) | 2 hours |
| Breast milk | 4 hours |
| Infant formula | 6 hours |
| Non-human milk (cow, goat) | 6 hours |
| Light meal (toast, clear soup) | 6 hours |
| Full meal (fried foods, fatty meat) | 8 hours or longer |
The counting of the fasting period begins at the time of ingestion, not at the time the meal concludes. A patient who finishes a heavy meal at midnight should not undergo an epidural procedure before 8:00 AM at the earliest.
Consequences of Non-Compliance
Scheduled procedures may be delayed or canceled entirely if a patient admits to eating outside the fasting window. This cancellation occurs not as a punishment but as a risk mitigation strategy.
The surgical team cannot safely proceed when the risk of aspiration outweighs the benefits of the planned intervention. Patients who do not disclose their recent food intake place themselves at serious medical risk.
The anesthesiologist may proceed with the case under false pretenses, believing the airway to be protected. Emergency airway management in a patient with a full stomach is technically difficult and carries a higher rate of complications including hypoxia and cardiac events.
3. Drinks and Fluids Before the Procedure
The rules governing liquid intake differ significantly from those applied to solid food. Clear fluids empty from the stomach rapidly, typically within one to two hours, which creates a different risk profile.
The stomach treats a glass of water much differently than it treats a cheeseburger. The purpose of allowing certain fluids while restricting others relates directly to gastric emptying rates and particulate matter.
Clear Liquids
Clear liquids are defined by their transparency at room temperature and their lack of solid content. These beverages leave the stomach rapidly and do not require digestion before absorption.
The two-hour fasting rule for clear liquids allows patients to remain hydrated and comfortable before a procedure.
- Water: Plain water represents the safest option and can be consumed in small amounts up to two hours before the procedure.
- Apple juice: This juice lacks pulp and passes through the stomach similarly to water despite its sugar content.
- White grape juice: Like apple juice, this option contains no particulate matter and leaves minimal gastric residue.
- Black coffee or tea: Coffee consumed without milk, cream, or nondairy creamer qualifies as a clear liquid.
- Clear carbonated beverages: Sprite, ginger ale, and seltzer water are acceptable if they are free of pulp or coloring agents.
Patients should limit these fluids to small volumes rather than drinking large quantities right up to the cutoff time.
Problematic Beverages
Many beverages appear harmless but contain components that convert them into solid food equivalents inside the stomach. The stomach must process proteins and fats from dairy products before emptying can occur.
Sugary liquids with high osmolality can also delay gastric emptying compared to plain water.
- Milk and cream: Dairy products contain casein and whey proteins that coagulate in the acidic stomach environment.
- Fruit smoothies: These drinks contain fiber, seeds, and pulp that require mechanical and enzymatic breakdown.
- Orange juice with pulp: Even small amounts of pulp represent particulate matter that can obstruct the airway if aspirated.
- Protein shakes: These formulated beverages often contain thickeners and protein isolates that behave like a light meal.
- Alcoholic beverages: Alcohol irritates the gastric mucosa and can affect patient cooperation and consent.
A patient who drinks orange juice with pulp has effectively eaten oranges. The stomach cannot distinguish between chewed fruit and blended fruit once the material arrives for processing.
Hydration and Medication Swallowing
Patients frequently require sips of water to take essential medications on the morning of a procedure. This practice is generally acceptable and does not violate fasting protocols when performed correctly.
The anesthesiologist needs to know about any medications taken and the volume of water consumed.
- Essential medications: Blood pressure medications, thyroid replacements, and seizure drugs should typically be taken as scheduled.
- Small sips: One or two ounces of water to facilitate swallowing does not significantly increase gastric volume.
- Timing: Medications should be taken at least two hours before the procedure when possible to allow gastric emptying.
Patients should verify medication instructions with their physician rather than making assumptions about safety. Some medications interact with anesthetic agents or affect coagulation in ways that require special consideration.
4. Unfamiliar or Recreational Substances
The anesthesiologist administers epidural medications with a specific dose-response relationship in mind. Recreational drugs introduce unpredictable variables into this equation, as their composition and potency remain unknown.
A patient's system may contain substances that amplify, diminish, or dangerously interact with the standard anesthetic agents. These interactions can manifest during the procedure or emerge during the recovery period.
Drug Interactions and Anesthetic Complications
Recreational substances exert their effects through various neurotransmitter systems and receptor pathways. These neurochemical alterations do not simply disappear when anesthetic agents are introduced.
The resulting combination can produce cardiovascular instability, respiratory depression, or prolonged sedation.
- Stimulants (cocaine, methamphetamine, MDMA): These drugs increase circulating catecholamines and can cause severe hypertension or cardiac arrhythmias when combined with certain anesthetics.
- Opioids (heroin, fentanyl, prescription pain relievers): Chronic opioid use leads to tolerance and may render standard epidural analgesia ineffective.
- Cannabis: Regular cannabis users often require higher doses of sedatives and anesthetics to achieve the desired effect.
- Benzodiazepines (Xanax, Valium obtained illicitly): These drugs potentiate the effects of anesthetic agents and can lead to prolonged sedation and respiratory depression.
- Hallucinogens (LSD, psilocybin): These substances can alter perception and may contribute to emergence delirium or panic during the procedure.
The anesthesiologist adjusts medication selection and dosing based on the substances present in the patient's system. This adjustment cannot occur without accurate information about recent use.
Disclosure and Safety
The preoperative period represents the ideal time for honest discussion regarding substance use. Patients who fear judgment or legal consequences should understand that medical privacy laws protect their information.
The anesthesia team does not contact law enforcement or report lawful medical information to outside agencies.
- Direct questioning: The anesthesiologist asks about substance use specifically to plan a safe anesthetic, not to interrogate the patient.
- Timing matters: Information about recent use, particularly within the last 24 to 48 hours, carries the greatest significance for anesthetic planning.
- Withdrawal risk: Patients dependent on alcohol, opioids, or benzodiazepines may experience withdrawal during the perioperative period if this information remains undisclosed.
The anesthesia team can provide medications to prevent withdrawal symptoms and ensure patient comfort. Undisclosed substance use eliminates this possibility and forces the medical team to react to symptoms rather than prevent them.
Conclusion
An epidural injection requires careful preparation that extends beyond simply arriving at the hospital on time. The substances a patient introduces into their body or applies to their skin directly influence the safety and success of the procedure.
Patients who follow preoperative instructions provide the anesthesiologist with optimal conditions for needle placement. Clear communication regarding all medications, supplements, and substances ensures accurate dosing and appropriate agent selection.
Safe outcomes depend on the partnership between patient and physician during the preparation phase. The information provided here represents general guidelines that apply to most patients in most situations.
When your child lives with ongoing pain, parenting begins to look very different from what you once imagined. School mornings may feel uncertain. Sleep can become inconsistent. Plans often revolve around flare ups rather than calendars. Parenting a child with chronic pain means learning how to support physical comfort while also protecting emotional wellbeing and long term independence.

The goal is not simply to eliminate discomfort, but to help your child function, grow, and build resilience despite it. With structure, informed medical care, and intentional parenting strategies, families can create stability even when symptoms are unpredictable. Let's look at strategies for parenting a child with chronic pain.
Understanding Chronic Pain in Children
Chronic pain in children is typically defined as pain lasting longer than three months. It may be associated with conditions such as migraines, juvenile idiopathic arthritis, functional abdominal pain disorders, inflammatory conditions, or sickle cell disease. In many cases, pain persists even after the original injury or illness has healed.
The Centers for Disease Control and Prevention notes that chronic health conditions affect a significant number of children in the United States, and persistent pain is one of the most challenging symptoms families face.
Chronic pain is not simply prolonged discomfort. It involves changes in how the nervous system processes pain signals, which can make the body more sensitive over time. This means that even minor triggers may feel intense. The pain is real, even when imaging or laboratory results appear normal.
Children express pain differently depending on their age and personality. Younger children may become irritable, clingy, or withdrawn. School aged children may avoid activities they once enjoyed. Teenagers may struggle with mood changes or social isolation. Recognizing these behavioral shifts helps parents respond with empathy instead of frustration.
Common Pediatric Chronic Pain Conditions
Some commonly diagnosed conditions include:
- Chronic migraines or tension headaches
- Juvenile idiopathic arthritis
- Functional abdominal pain disorders
- Sickle cell related pain crises
Although the medical causes differ, the daily impact often overlaps. Children may miss school, struggle with sleep, avoid sports, or withdraw from friendships. Over time, these disruptions can affect confidence and academic progress.
Understanding the condition itself is only the first step. The next challenge is building a home environment that supports both healing and normal development.
Creating Stability in an Unpredictable Situation
When pain levels change from day to day, structure becomes incredibly important. A predictable routine reduces stress, and stress can increase pain sensitivity. The American Academy of Pediatrics emphasizes the importance of maintaining daily function and normal routines as part of pediatric chronic pain care.
Consistency in daily structure provides children with a sense of control when their bodies feel unpredictable. Establish regular times for waking, meals, homework, and bedtime. Even if adjustments are occasionally necessary, the routine itself offers reassurance.
A written pain action plan can also reduce uncertainty. This plan may include early warning signs of flare ups, preferred coping strategies, medication timing, and clear guidelines on when to contact a healthcare provider. Having this plan visible in the home removes guesswork during stressful moments.
Encouraging Activity Without Overprotection
One of the most difficult balances in parenting a child with chronic pain is knowing when to push gently and when to step back. It is natural to want to shield your child from discomfort. However, complete avoidance of activity can unintentionally increase disability and fear.
Encourage gradual participation in school, social events, and hobbies. Modifications may be necessary. A child with joint pain might choose swimming instead of contact sports. A teen with migraines may require scheduled rest breaks during school.
Instead of asking whether something hurts too much to try, consider asking what would make the activity manageable. This small language shift promotes problem solving rather than avoidance.
Supporting Restorative Sleep
Sleep and pain are closely connected. Inconsistent sleep can heighten pain sensitivity, while chronic pain can disrupt sleep cycles. Establishing calming bedtime routines is critical. Limit screen exposure before bed, maintain consistent sleep and wake times, and create a quiet environment.
Healthy sleep supports hormonal regulation, immune function, and emotional stability. Even small improvements in sleep hygiene can positively influence overall pain management.
Working Effectively With Healthcare Providers
Chronic pain often requires a multidisciplinary approach. Pediatricians may coordinate care with pain specialists, physical therapists, psychologists, or other specialists depending on the diagnosis. The National Institute of Neurological Disorders and Stroke supports comprehensive approaches that address both physical and psychological components of pain.
Open communication with healthcare providers turns uncertainty into informed decision making. Keep a detailed record of pain episodes, triggers, sleep patterns, and medication effects. Patterns often emerge over time, helping providers refine treatment strategies.
As children grow older, encourage them to participate in appointments. Adolescents especially benefit from practicing how to describe symptoms and ask questions. This builds confidence and prepares them for adult healthcare systems later in life.
Common Components of Treatment
Treatment typically combines several strategies rather than relying on a single solution.
| Treatment Approach | Purpose | Benefit | Consideration |
| Medication | Reduce inflammation or nerve sensitivity | May decrease flare intensity | Requires monitoring |
| Physical Therapy | Improve mobility and strength | Supports long term function | Needs consistency |
| Psychological Support | Build coping strategies | Reduces fear and anxiety around pain | Works best with family support |
| Lifestyle Adjustments | Improve sleep, stress control, nutrition | Supports overall regulation | Requires daily commitment |
This integrated model recognizes that chronic pain affects the whole child, not just one body part.
Navigating School Accommodations
Children with persistent pain may experience increased school absences. Without a plan, this can lead to academic stress and social isolation.
Meet with school administrators to discuss possible accommodations. These might include flexible deadlines, modified physical education requirements, rest breaks, or access to the school nurse. Clear communication prevents misunderstandings and ensures your child feels supported rather than punished for a medical condition.
Gradual return to full participation after prolonged absences can also ease anxiety. A phased schedule may help rebuild stamina and confidence.
Supporting Emotional Health
The emotional toll of chronic pain can be significant. Frustration, anxiety, sadness, and even anger are common responses. When children feel different from peers, isolation may follow.
Validating your child’s emotional experience strengthens resilience and prevents long term withdrawal. Avoid minimizing statements, even if they are meant to comfort. Instead, acknowledge feelings and collaborate on coping strategies.
Teaching Coping Tools
Children benefit from learning practical self regulation skills. Deep breathing, progressive muscle relaxation, guided imagery, journaling, and gentle stretching are common tools. Some families create a comfort corner at home with heating pads, soft blankets, or calming music.
Encourage your child to reflect on what has helped during past flare ups. Over time, this builds a sense of mastery. The message becomes clear: pain may occur, but there are strategies available.
Peer support groups, whether in person or virtual, can also reduce isolation. Connecting with others who understand chronic illness helps normalize the experience.
Considering Family Dynamics
Chronic illness affects siblings and caregivers as well. Brothers and sisters may feel overlooked or confused. Open conversations about fairness and emotional needs are important.
Schedule individual time with siblings when possible. Even brief, focused attention reinforces their importance within the family system. Including them in age appropriate discussions about the condition can also reduce misconceptions.
Preparing for Long Term Independence
As children move into adolescence, the focus gradually shifts toward self management. Teaching teens to track medications, schedule appointments, and understand their condition builds independence.
Transitioning from full parental control to guided independence is a gradual but essential process. Allow teens to take increasing responsibility under supervision. Encourage them to communicate directly with teachers and healthcare providers.
Planning for college or employment may involve exploring accommodations or flexible scheduling options. With preparation, many young adults with chronic pain pursue higher education and meaningful careers.
Financial considerations may also arise over time. Consulting with insurance representatives or hospital social workers can provide clarity about coverage and long term planning.
Caring for Yourself as a Parent
Caring for a child with chronic pain can be emotionally exhausting. Parents often operate in constant vigilance mode, anticipating the next flare up. Over time, this stress can accumulate.
Your wellbeing directly affects your child’s emotional stability, making self care a necessity rather than a luxury. Seek support from trusted friends, counseling services, or parent groups. Accept help when offered. Even small breaks can restore perspective.
Maintain open communication with co parents or other caregivers. Aligning on routines and expectations reduces conflict and creates consistency for your child.
Modeling healthy coping behaviors, such as exercise, balanced nutrition, and emotional expression, sends a powerful message.
Parenting a Child with Chronic Pain
Parenting a child with chronic pain is not about eliminating every difficult day. It is about creating an environment where your child feels understood, supported, and capable. Pain may remain part of their life, but it does not have to define their identity or limit their potential.
As children grow, new questions naturally emerge about long term planning, higher education, employment, and independent healthcare management. Exploring how families can guide adolescents toward confident self advocacy becomes the next important conversation in supporting children who grow up navigating persistent pain.
Chronic pain affects millions of older adults, and families often struggle to know how much relief is truly possible. Many seniors describe pain as something they are expected to “just live with,” yet modern care offers far more supportive options than most people realize.
This article explores practical strategies that blend medical guidance, lifestyle improvements, home modifications, and emotional support in ways that can meaningfully improve day-to-day comfort. By bringing together the most effective approaches, it becomes easier to understand what responsible care looks like and how to adapt it as needs evolve.

These insights help caregivers make informed decisions and help seniors maintain dignity, independence, and a higher quality of life. Let's look at the practical tips for managing chronic pain in the elderly.
Understanding Chronic Pain in Older Adults
Pain in older adults does not occur in a vacuum. Most seniors live with several ongoing medical conditions at once, making it harder to identify what is causing discomfort at any given moment.
That is why early conversations with healthcare providers matter so much. The more thoroughly someone describes the location, timing, and intensity of their symptoms, the more accurately a clinician can pinpoint the source.
Many of the most common pain triggers in later life are cumulative. Osteoarthritis gradually wears away cartilage, neuropathy affects nerve communication, and spinal stenosis narrows the spaces where nerves travel.
Each condition creates a unique type of discomfort that responds best to different interventions. Families often assume two types of pain are the same, even when they require completely different treatments.
Taking time to understand the underlying cause of pain sets up every future decision for greater success.
Common Sources of Pain in Older Adults
- Joint degeneration such as osteoarthritis
- Diabetic or idiopathic neuropathy
- Chronic back pain, spinal stenosis, disc degeneration
- Pain following surgery or joint replacement
- Long term inflammatory conditions
These conditions often overlap, and seniors frequently underreport symptoms because they worry about being a burden. Encouraging honest communication helps prevent misdiagnosis and ensures clinicians have enough information to recommend appropriate care.
How Aging Changes Pain Perception
An aging body processes pain differently. Nerves fire more slowly, and some pain signals may be dulled while others feel unusually intense.
Healing also takes longer, which means minor injuries can evolve into chronic issues. This shift makes diagnostic evaluations more complicated but reinforces the value of early attention.
Why Diagnosis Is Sometimes Difficult
Multiple medications, cognitive changes, and overlapping health problems can mask important clues. Providers may rely on imaging, physical exams, and patient diaries to gather enough information to form a complete picture.
Accurate assessment remains the most important step in preventing unnecessary suffering.
Medical Strategies for Chronic Pain Relief
Medical treatments remain foundational tools in pain care, especially when symptoms interfere with sleep, mobility, or daily activities. While pain medications must always be used cautiously in older adults, there are several options that can safely support comfort when monitored properly.
Clinicians often begin with the least aggressive approach and work upward as necessary. Acetaminophen is commonly suggested for joint or muscle pain because it is gentler on the stomach than many anti-inflammatory drugs.
Topical creams and patches can also be effective for localized discomfort. Medication decisions should always consider a senior’s full list of prescriptions to avoid harmful interactions or duplications.
Commonly Used Medications in Older Adults
- Acetaminophen for baseline pain
- Topical lidocaine or anti inflammatory gels
- Anti inflammatory medications when appropriate
- Low dose antidepressants or anticonvulsants for neuropathic pain
Because many seniors metabolize drugs differently, providers typically adjust dosages more gradually and conduct follow up evaluations more frequently.
When Interventional Treatments Are Helpful
Some older adults experience relief from minimally invasive procedures such as joint injections, targeted nerve blocks, or epidural steroid treatments. These options can reduce inflammation, improve mobility, and decrease the amount of medication needed daily.
For individuals who struggle with side effects or cannot tolerate oral medications, these interventions can open the door to meaningful improvements in mobility and mood.
Why Routine Monitoring Matters
Pain levels naturally fluctuate, and medication needs may change after life events, surgeries, or new diagnoses. Regular appointments help prevent complications and allow providers to make timely adjustments.
Thoughtful medical supervision protects seniors from unnecessary risks and ensures their treatment remains aligned with their health goals.
Lifestyle Approaches That Support Comfort and Mobility
Lifestyle adjustments are often underrated, yet they create some of the most consistent improvements in long term comfort. Movement, sleep, and nutrition form a stable foundation for every other treatment.
Even small habit changes can reduce flare ups and restore a sense of control for seniors who feel overwhelmed by chronic symptoms.
Gentle Movement and Low Impact Exercise
Many older adults fear that exercise will worsen their pain, but supervised movement usually has the opposite effect. Physical therapists teach targeted exercises that build muscle strength, improve balance, and increase flexibility.
A regular walking routine, aquatic therapy, or seated chair exercises can reduce stiffness and support circulation. Movement helps break the cycle of inactivity, weakness, and worsening pain that often develops in later life.
To make routines easier to follow, consider structuring activities into short daily sessions rather than long workouts. This approach adds consistency without overwhelming the senior.
Establishing Sleep Habits That Reduce Pain Symptoms
Poor sleep has a direct impact on pain levels. A 2021 National Sleep Foundation survey found that adults who sleep fewer than six hours per night report significantly more pain interference during the day.
Encouraging consistent bedtimes, limiting caffeine late in the day, and creating a calming evening routine can reduce nighttime discomfort. Supportive pillows and a mattress suited to the senior’s needs also contribute to better rest.
Nutrition Habits That Support Pain Reduction
Even modest dietary changes can reduce inflammation. Many seniors benefit from:
- Increased hydration
- Balanced meals with fruits, vegetables, and lean proteins
- Omega 3 rich foods such as salmon or walnuts
- Reduced intake of highly processed foods
Digestive health also plays a role. Some medications cause dehydration or constipation, which may worsen discomfort in ways seniors do not always connect to their diet. A simple, steady nutrition plan strengthens the body’s ability to manage pain more effectively.
Home Modifications to Ease Daily Strain
Safety and comfort at home are essential for maintaining independence. Many pain flare ups occur during routine activities such as bathing, standing, or getting out of bed.
Small changes can dramatically reduce risk and strain.
Fall Prevention and Mobility Support
Falls often lead to new or worsening pain conditions. Installing grab bars in bathrooms, adding railings on stairs, and using non slip flooring can prevent injuries.
Nightlights help reduce disorientation when seniors get up in the dark.
Ergonomic Adjustments for Daily Activities
Modifications that reduce bending and twisting ease joint and muscle strain. Raised toilet seats, adjustable beds, repositioned kitchen items, and supportive chairs with proper height all make daily life smoother.
Improving lighting reduces eye strain and helps seniors avoid awkward or unsafe movements.
Assistive Devices That Make Mobility Easier
Devices such as walkers, canes, reachers, or long handled shoehorns reduce the physical effort required for basic tasks. These tools protect joints from unnecessary pressure and help seniors maintain independence without aggravating pain.
Designing a home that accommodates physical limitations empowers older adults to move more confidently and safely.
Emotional and Social Support in Pain Care
Chronic pain is not only physical. It affects confidence, mood, sleep, and motivation.
Seniors may withdraw from social activities or feel frustrated about relying on others. These emotional responses can intensify pain, creating a challenging cycle.
How Ongoing Pain Impacts Mood and Independence
Depression and anxiety are more common among older adults with chronic pain. When discomfort limits mobility or disrupts sleep, emotional effects accumulate.
Caregivers may notice changes in appetite, patience, or engagement with activities once enjoyed. Acknowledging emotional strain is a meaningful step toward restoring balance and well being.
The Role of Social Engagement
Regular interaction with friends, family, or community groups provides mental stimulation and emotional grounding. Programs at senior centers, adult day services, or faith based organizations offer companionship and purpose.
Social connections often distract from pain and help maintain routine, which in turn improves overall functioning.
Mind Body Techniques That Encourage Relaxation
Breathing exercises, gentle stretching, guided imagery, and mindfulness practices help quiet stress responses that intensify pain signals. Some seniors also benefit from supportive counseling, especially if pain has altered their lifestyle significantly.
These tools complement medical treatment and give seniors more control over their internal environment.
Practical Tips for Chronic Pain Management in the Elderly
This section incorporates the required primary keyword chronic pain management in the elderly exactly once. Practicality matters most when caregivers are trying to support someone day to day.
A structured plan makes it easier to track what works, identify what needs adjustment, and provide clinicians with helpful information.
Building a Personalized Care Plan
A holistic plan integrates medical, physical, emotional, and environmental strategies. Families often create a simple binder or digital document that includes medication schedules, exercise routines, sleep patterns, and symptom notes.
A clear record keeps everyone aligned and helps seniors feel more in control of their care.
Working With Healthcare Providers Effectively
Prepare questions ahead of appointments and note any changes in pain patterns. Bring updated medication lists and describe how pain affects daily activities rather than focusing solely on severity.
This context helps clinicians refine treatment in ways that match the senior’s lifestyle. Clear communication ensures that medical decisions reflect the senior’s actual needs rather than assumptions.
Knowing When to Reassess or Modify the Plan
Some signs that adjustments may be necessary include:
- New or spreading pain
- Increased difficulty walking or sleeping
- Declining appetite or mood
- Side effects from medications
- A noticeable drop in participation in daily activities
Reevaluation does not mean previous strategies failed. Instead, it reflects the natural changes that occur with aging. Over time, even well designed plans require updates.
Comparison Table: Approaches to Pain Management
| Approach | Benefits | Best For | Considerations |
| Medication management | Reduces acute or persistent pain | Joint pain, neuropathy, inflammation | Monitor for side effects and interactions |
| Physical therapy | Improves mobility and strength | Muscle weakness, arthritis | Requires consistency for best results |
| Home modifications | Reduces strain and fall risk | Limited mobility, balance problems | Some adjustments may require installation |
| Mind body techniques | Enhances relaxation and emotional balance | Stress related pain, sleep issues | Works best alongside other treatments |
Practical Tips for Managing Chronic Pain in the Elderly
This final section uses the main keyword in the heading as required. It reinforces earlier insights and prepares readers for deeper exploration of senior wellness topics.
Many families find that addressing chronic pain is an ongoing process rather than a single solution, and understanding this perspective helps reduce frustration for everyone involved.
Practical strategies often work best when adopted gradually. For example, introducing a walking routine twice a week may feel more achievable than daily exercise at first.
Home safety changes can start with lighting improvements before more involved renovations. Emotional support can begin with simple check ins or short conversations that encourage seniors to share their experiences.
Small, steady improvements create meaningful shifts in comfort and confidence.As seniors adapt to new routines, caregivers can observe which strategies seem to offer the greatest benefit.
This observational approach leads naturally into broader wellness topics such as fall prevention, mobility training, and support for long term independence. Exploring these areas can help families build a proactive plan that supports not only pain relief but also quality of life.
Shooting pain behind the knee can arise from various causes, often related to injuries or underlying medical conditions. Common culprits include Baker's cysts, which are fluid-filled sacs that develop due to joint fluid accumulation, often linked to arthritis or meniscus tears.
Injuries such as hamstring strains, posterior cruciate ligament (PCL) tears, or meniscus injuries can also lead to sharp pain. Additionally, conditions like osteoarthritis and deep vein thrombosis (DVT) may contribute to discomfort. Symptoms can vary from sharp and sudden pain to swelling and stiffness, necessitating a proper diagnosis for effective treatment. Let's look at causes of shooting pain behind the knee.
Common Causes of Pain Behind the Knee
Pain behind the knee can result from various medical conditions or injuries. This discomfort may stem from structural issues within the knee joint, inflammation, or underlying systemic conditions. Understanding the potential causes can help guide diagnosis and treatment, promoting recovery and long-term health.

1. Baker’s Cyst
A Baker's cyst, or popliteal cyst, is a fluid-filled swelling behind the knee caused by the buildup of synovial fluid. This occurs when the knee joint produces excess fluid due to underlying conditions like arthritis or a meniscus tear.
Symptoms of a Baker’s cyst often include noticeable swelling and tightness in the back of the knee, particularly when bending or straightening the leg. The discomfort can intensify after physical activity. While a cyst is not inherently dangerous, it may rupture in rare cases, causing sudden, sharp pain and bruising in the calf.
2. Injuries
Several injuries can result in pain in the knee. The most common include:
Hamstring Injury
The hamstring is a group of muscles running along the back of the thigh. These muscles are crucial for knee flexion and hip extension. Hamstring injuries often occur during activities that involve sprinting, jumping, or sudden directional changes.
A hamstring strain or tear can lead to pain radiating from the thigh to the back of the knee. The severity of the injury varies, ranging from mild overstretching to a complete muscle tear. Swelling, bruising, and weakness in the affected leg are common symptoms.
Meniscus Tear
The meniscus is a cartilage structure that acts as a cushion and stabilizer in the knee joint. Tears in the meniscus often occur due to twisting motions during activities like sports.
Symptoms of a meniscus tear include pain, swelling, and a feeling of instability in the knee. A tear in the posterior region of the meniscus can lead to significant pain behind the knee, especially during movements like squatting or kneeling.
Posterior Cruciate Ligament (PCL) Injury
The posterior cruciate ligament (PCL) is one of the key stabilizers of the knee. Injuries to the PCL often result from direct trauma, such as hitting the knee against a dashboard in a car accident or landing awkwardly during sports.
Pain behind the knee is a hallmark symptom of PCL injuries. Swelling, stiffness, and difficulty walking are also common, with severe injuries causing instability in the joint.
3. Arthritis
Arthritis refers to inflammation of the joints, and it can significantly impact the knee. The two most common types affecting the knee are osteoarthritis and rheumatoid arthritis.
Osteoarthritis
This is a degenerative condition characterized by the gradual breakdown of cartilage in the knee joint. It often develops with age or repetitive use of the joint. Symptoms include stiffness, swelling, and varying degrees of pain that may worsen after activity or prolonged sitting.
Rheumatoid Arthritis
This is an autoimmune disorder where the immune system attacks healthy joint tissue. It causes inflammation, swelling, and tenderness. Rheumatoid arthritis often leads to persistent discomfort and deformity if untreated. Pain behind the knee can be especially noticeable during flare-ups.
4. Deep Vein Thrombosis (DVT)
Deep vein thrombosis (DVT) is a serious condition caused by a blood clot forming in the deep veins of the leg, often behind the knee. It poses significant risks, as the clot can travel to the lungs and cause a life-threatening pulmonary embolism.
Symptoms of DVT include swelling in the affected leg, warmth, redness, and severe pain behind the knee or calf. Individuals with risk factors such as prolonged immobility, recent surgery, or clotting disorders should seek immediate medical attention if DVT is suspected.
5. Tendinitis
Tendinitis refers to inflammation of the tendons around the knee, particularly those in the hamstrings or the popliteus tendon. It is commonly caused by overuse, repetitive motions, or sudden increases in activity.
Sharp or burning pain, especially during movement or physical exertion, is a primary symptom. Swelling and tenderness may also accompany the pain. Proper rest and physical therapy are often effective in managing tendinitis.
6. Bursitis
The bursae are small, fluid-filled sacs that cushion the joints and reduce friction between tissues. Bursitis occurs when these sacs become inflamed, often due to repetitive stress, direct trauma, or prolonged kneeling.
Pain from bursitis is typically localized and improves with rest. Other symptoms include swelling and tenderness around the back of the knee. Chronic bursitis can lead to stiffness and discomfort during movement.
7. Infections
Infections affecting the knee, such as septic arthritis, can lead to severe pain behind the knee. These infections may occur due to bacterial invasion of the joint space, often after an injury, surgery, or bloodstream infection.
Symptoms of an infected knee include redness, warmth, swelling, fever, and intense pain. These symptoms require prompt medical intervention to prevent permanent joint damage or systemic complications.
8. Tumors
Though rare, tumors near the knee can be a cause of persistent pain. Both benign and malignant tumors, such as osteosarcomas, can develop in or around the joint.
Persistent pain, noticeable swelling, and visible deformities are potential signs of a tumor. While benign tumors may not always require intervention, malignant growths necessitate prompt diagnosis and treatment.
Less Common Causes of Pain Behind the Knee
While less common, certain conditions can also lead to pain behind the knee. These include fractures, compressed nerves, and leg cramps. Understanding these causes can help identify and address the underlying problem effectively.
1. Fractures
Fractures in the knee area can occur due to direct trauma, such as a fall, car accident, or sports injury. These fractures may involve bones like the tibia, fibula, or patella.
Symptoms of a knee fracture include severe pain, swelling, bruising, and an inability to bear weight on the affected leg. The deformity may also be present in severe cases. Immediate medical attention is necessary to prevent complications and ensure proper healing.
2. Compressed Nerves
Nerve compression in the lower back or hip can lead to referred pain in the knee. Sciatica, for instance, occurs when the sciatic nerve is compressed, causing radiating pain down the leg.
Symptoms of nerve compression include tingling, numbness, or burning sensations in the leg, along with pain behind the knee. Prolonged sitting, poor posture, or herniated discs are common triggers. Treatment often involves physical therapy, posture correction, and sometimes medical intervention.
3. Leg Cramps
Leg cramps, particularly in the hamstrings, can cause sudden, acute pain behind the knee. These involuntary muscle contractions are often triggered by dehydration, muscle fatigue, or electrolyte imbalances.
Symptoms of leg cramps include sharp pain and tightness in the back of the thigh. The pain is typically temporary but can linger if the cramp is severe. Staying hydrated, stretching, and ensuring adequate intake of essential minerals like potassium and magnesium can help prevent cramps.
Stabbing Or Sharp Knee Pain That Comes and Goes
Understanding the causes of stabbing or sharp knee pain that comes and goes is essential for effective management and relief. Whether it stems from injuries, such as ligament tears or strains, or conditions like Baker's cysts and osteoarthritis, recognizing the symptoms can help you seek timely medical attention.
If you experience persistent or severe pain, it's crucial to consult a healthcare professional for an accurate diagnosis and tailored treatment plan. By addressing the underlying issues, you can regain mobility and improve your quality of life, allowing you to return to the activities you enjoy without discomfort.
An old scar that begins to hurt feels like a ghost from a wound you thought had finished healing. The tissue is no longer an open injury, yet it sends a clear message that something beneath the surface is not at rest.
This late-onset pain signals altered tissue that now behaves differently from the surrounding skin and muscle. The original injury severed blood vessels and nerve endings, forcing the body to weave a hasty bridge of collagen fibers to close the gap.
The scar is disorganized and less elastic than the tissue it replaced, creating a fixed point that cannot move normally. As surrounding muscles tighten with age or new physical demands arise, that rigidity becomes a source of radiating tension and pain. Why does my scar hurt years later and what you can do about it? Let's look into it.
The Main Reasons for Old Scar Pain
Nerve endings trapped within that fibrous patch can misfire, generating sharp sensations or a deep, persistent ache as they respond to pressure or chemical changes in the environment. The scar tissue itself may even develop trigger points, acting as a knot that refers pain to distant parts of the body.

- The Nerve Reorganization Process
A deep cut or surgical incision does not simply divide skin. It severs the intricate network of sensory nerves that branch through the tissue.
During healing, the body works to seal the wound, but the nerve ends do not always reconnect in an orderly fashion. They can form what doctors call a neuroma, a tangled cluster of sprouting nerve fibers trapped within the collagen of the scar.
This disorganized nerve tissue becomes highly sensitive to mechanical pressure. A light brush of clothing or a change in the weather can compress these trapped endings, which then fire off signals interpreted by the brain as pain.
The sensation can present as a sharp electric shock, a persistent burning feeling, or the odd pins-and-needles prickle that radiates out from the scar line. These nerves can remain dormant for years before some new stimulus finally triggers them.
- The Adhesion of Deeper Layers
Scar tissue does not confine itself to the surface. It extends downward, binding the skin to the layers of fat, fascia, and muscle beneath it.
This binding creates adhesions, which anchor the skin firmly to the structures underneath. Normal tissue slides and glides with body movement; an adhesion pulls and tugs.
When you bend a joint or stretch a muscle near an old scar, that anchored spot cannot move with the rest of the body. The tension concentrates directly on the scar, creating a sharp pulling sensation or a deep ache.
This is why a scar on the lower back might throb after a day of bending or why a scar near the shoulder can make reaching for a high shelf unexpectedly painful. The adhesion turns every stretch of the surrounding tissue into a direct pull on the scar itself.
- The Collagen Structure Disorganization
Healthy skin contains collagen woven in a basket-weave pattern, which provides strength and flexibility. A scar forms rapidly, with the body laying down collagen in thick, parallel bundles to close the wound quickly.
This structure resembles a mound of hastily stacked sticks rather than a woven basket. The parallel alignment creates a patch of tissue that is significantly less elastic than the surrounding dermis.
It cannot deform and rebound under stress. When the body moves, the rigid scar tissue acts as a stress riser, a point where force concentrates rather than dissipates.
- The Latent Inflammatory Response
Inflammation is the initial step of wound healing, a cascade of cellular activity that cleans the injury and builds new tissue. In some cases, this inflammatory process does not fully switch off.
It can settle into a low-grade, chronic state within the scar tissue, flaring up years later under the right conditions. Minor trauma to the area, such as a bump or a hard workout, can reactivate these latent immune cells.
The body may respond as if the original wound has been reopened, flooding the site with chemicals that cause swelling and tenderness. This explains why an old scar can suddenly become puffy, red, or sore to the touch for no apparent reason, only to settle down again after a period of rest.
Everyday Things That Can Flare Up a Scar
The scar on your body is not a static monument to an old injury. It is living tissue that responds to how you move, how you sit, and how you care for it.

The pain it produces is a signal worth listening to, and with the right approach, it is a signal you can quiet.
- Weather Shifts and Atmospheric Pressure
The dense, fibrous tissue of a scar does not respond to atmospheric changes in the same way as normal skin. When barometric pressure drops before a storm, the surrounding tissues expand slightly.
The effect is most pronounced during cold weather, as low temperatures can also cause muscles to tense and contract.
- A drop in humidity can dry out the scar tissue itself, making it less pliable and more prone to cracking or irritation.
- Many individuals report that their scars serve as reliable predictors of rain, aching hours before any precipitation falls.
The scar tissue, with its tight collagen structure, cannot expand with them. This discrepancy creates a physical pull on the nerve endings embedded within the scar.
- Repetitive Motion and Physical Stress
A scar that has been quiet for years can suddenly protest when introduced to a new pattern of movement. The tissue has adapted to a certain range of motion, a specific set of daily demands.
When that range is exceeded or changed, the scar becomes the weakest link in the kinetic chain.
- Starting a new exercise routine, such as running or weightlifting, can place unfamiliar tensile forces on an old scar.
- Occupational tasks that require repetitive bending, lifting, or twisting can gradually irritate the adhesion points.
Even a change in posture or gait, perhaps from a new pair of shoes or a minor back injury, can alter how the tissue around the scar is pulled throughout the day.
- Prolonged Periods of Inactivity
Sitting at a desk or lying in bed for extended hours allows the tissues to settle into a static position. Muscles shorten, fascia tightens, and the scar tissue loses the small amount of movement it normally experiences.
When a person finally stands up and moves, the sudden stretch on these shortened structures pulls sharply on the scar. This explains the common complaint of pain upon standing after a long car ride or a night of sleep.
The scar and the tissue around it have essentially stiffened in place. The first movement of the day or after a long rest requires the scar to stretch abruptly, which it cannot do without signaling pain.
- Psychological Stress and Muscle Tension
The body holds emotional tension in specific muscle groups, commonly the jaw, the neck, the shoulders, and the lower back. If a scar resides in one of these high-tension zones, it becomes a passive recipient of that stress.
The brain may send a signal to brace for a stressful situation, which causes the muscles to contract around the scar.
- Chronic anxiety can lead to a permanent state of low-level muscle tension, constantly pulling on the scar tissue.
- During periods of high stress, individuals may also unconsciously touch or rub the area, adding mechanical irritation to the existing muscle tension.
The scar can become a somatic focal point, a physical location where the psychological state manifests as tangible discomfort.
- Nutritional and Hydration Changes
The health of all tissue, including scar tissue, depends on adequate hydration and nutrition. When the body becomes dehydrated, every tissue loses some of its fluid content.
Skin loses elasticity, and the dense collagen of a scar becomes even more rigid and brittle.
- A diet low in essential fatty acids can impair the tissue's natural lubrication, making scars feel tighter.
- Deficiencies in vitamins C and D, which play roles in collagen maintenance, can affect the structural integrity of the scar matrix.
Significant weight gain or loss can stretch or shrink the skin around a scar, changing the tension dynamics and irritating the fixed point of the scar tissue.
How to Find Relief
Some resist home treatment. They hold their tightness or generate pain that spreads beyond their borders.
In these cases, professional help offers tools that go deeper than what the fingers can provide. A physical therapist or physician can identify the specific structures involved and apply treatments that break the cycle of chronic irritation.
- Daily Mobilization Techniques
The goal of scar mobilization is to restore movement between the layers of tissue that have become glued together. This requires direct, manual intervention to break the adhesions and encourage the collagen fibers to realign in a more flexible pattern.
The skin over a healthy scar should move freely over the muscle and fascia beneath it.
- Use the pads of two or three fingers to locate the tightest spot along the scar line.
- Press down gently until you feel resistance, then move the skin in small circles clockwise and counterclockwise.
- Pinch the scar between thumb and forefinger and lift it away from the underlying muscle, holding for a few seconds before releasing.
- Stretch the skin on either side of the scar in opposite directions, creating a transverse pull across the scar line.
These movements should be performed daily for several minutes. The sensation should be one of firm pressure and stretching, not sharp pain. Over time, this mechanical stress signals the fibroblasts to remodel the collagen into a more organized, flexible structure.
- Directed Stretching Protocols
A scar that crosses a joint or lies over a major muscle group requires specific stretching to maintain range of motion. The stretch must target the tissue planes that the scar has tethered, lengthening them gradually to reduce tension.
Without this directed input, the scar will continue to act as a brake on normal movement.
- Identify the movements that reproduce the pulling sensation around the scar.
- Move the joint or muscle slowly to the point where the pull is felt, then hold the position for a slow breath.
- Inhale deeply, and on the exhale, attempt to move just slightly further into the stretch.
- Repeat this cycle several times, allowing the tissue to relax incrementally with each breath.
Consistency matters more than intensity with this approach. A gentle, sustained stretch performed daily produces better long-term results than an aggressive stretch performed occasionally.
- Thermal Therapy Application
Temperature manipulation can alter the mechanical properties of scar tissue and the muscle tension around it. Heat and cold serve different purposes and should be selected based on the specific quality of the pain.
Apply a warm compress or heating pad to the area before mobilization or stretching. The heat increases blood flow and makes the collagen fibers more pliable, allowing for greater movement with less risk of irritation.
Use a warm soak in a bath to heat a large area around the scar, relaxing all the surrounding muscles at once. Apply an ice pack or a cold gel pack to the scar after activity if it feels hot, throbbing, or acutely irritated.
Conclusion
An old scar that hurts is a logical consequence of the body's remarkable but imperfect repair process. The tissue bridging the original wound lacks the elasticity and organization of healthy skin, and it responds to tension, weather, and movement in predictable ways.
The pain serves as a messenger, indicating that something in that local environment has changed or reached a limit. The path to relief begins with recognizing that the scar remains an active part of the body's mechanical system.
It can be stretched, mobilized, and hydrated. It can adapt to new demands if given the right input over time. Simple daily attention to the tissue often produces gradual but lasting improvement, returning the scar to a state of quiet function.
The sacroiliac joints form the critical mechanical link between the spine and the pelvis, transferring all gravitational forces from the upper body to the lower extremities. Their unique, limited range of motion provides essential stability for the entire lumbar-pelvic region during movement.
Despite their structural importance, these joints are a frequently underestimated source of chronic pain, commonly misattributed to lumbar disc pathology or hip osteoarthritis. Accurate recognition of the specific symptomatic pattern is the first necessary step toward effective clinical intervention.
Pain originating from these articulations presents with a distinct and reproducible set of sensory and mechanical characteristics. Identifying these clinical markers allows for differentiation from other musculoskeletal conditions with similar regional presentations. Below are sacroiliac joint pain symptoms you should recognize.
The Main Sign... Pain in a Very Specific Spot
The most reliable indicator of sacroiliac joint dysfunction is pain that localizes to a precise anatomical region. Unlike the diffuse ache of muscular strain or the radiating pain of neurogenic conditions, SI joint pain consistently presents over the joint itself.
Finding Your "Dimple Point"
Clinicians often refer to the posterior superior iliac spine, a bony landmark that correlates with the common dermal dimples found just lateral to the sacrum. The SI joints reside directly beneath this point.
This location is several centimeters lateral to the midline spinous processes of the lower lumbar vertebrae, a key distinction from central discogenic pain. Pain elicited by direct pressure over this specific landmark, particularly when it replicates the patient's primary complaint, provides strong diagnostic evidence for an SI joint etiology.
The "One-Sided" Clue
While bilateral involvement occurs, especially in systemic inflammatory conditions, mechanical SI joint dysfunction typically manifests unilaterally. This lateralized presentation stems from asymmetrical loading or a specific inciting injury that alters the mechanics of a single joint.
The resultant pain remains predominantly on the affected side, though compensatory mechanisms can sometimes create secondary discomfort on the contralateral side over time. This one-sided predominance helps differentiate it from many forms of central spinal stenosis or systemic back pain.
Pain That Stays Put
The referral pattern of SI joint pain further distinguishes it. The discomfort may radiate, but its epicenter remains anchored to the joint.
Patients can usually isolate the primary source with a single fingertip, a clinical sign known as the "finger test."
- The characteristic radiation patterns include the ipsilateral buttock, the posterior thigh, and occasionally the groin region.
- Pain that extends below the knee, or is accompanied by true neurologic symptoms like numbness or muscle weakness, suggests a different or concomitant pathology, such as lumbosacral radiculopathy.
- This stable, locatable quality contrasts sharply with the migrating or shooting pain associated with nerve root compression.
How the Pain Feels and When it Strikes
The qualitative nature of SI joint pain and its temporal relationship to specific activities form a critical part of its clinical profile. This pain is not a constant, uniform sensation but a dynamic experience defined by its mechanical triggers and variable intensity.
- A Deep, Dull Ache That Can Sharpen
Patients frequently describe a persistent, deep-seated ache within the buttock and pelvic region, which can be difficult to localize precisely at rest. This baseline discomfort originates from the joint's deep anatomical position and the surrounding ligamentous structures.
The pain characteristically transitions to a sharp, stabbing, or even gripping sensation during movements that directly load or torque the joint. This shift from a dull ache to acute pain with specific provocation is a hallmark feature, indicating mechanical stress on inflamed or dysfunctional articular and periarticular tissues.
- Pain That Worsens with Simple Activities
Aggravation by specific, common weight-bearing and transitional movements provides strong diagnostic clues.
- Standing from a Seated Position: This action places immediate, unilateral load on the SI joint as the body weight shifts. The transition often requires a forceful contraction of the gluteal muscles, which attach directly to the sacrum and ilium, further compressing the joint.
- Stair Climbing or Walking on an Incline: These activities demand repeated single-leg stances with a propulsive force, maximally engaging the kinetic chain that relies on SI joint stability.
- Prolonged Standing or Walking: Even level-ground ambulation can become problematic, as the repetitive minor rotations and shear stresses accumulate, leading to increasing pain and a consequent antalgic gait.
- Lying on the Affected Side: Direct pressure on the inflamed joint structures during sleep can provoke pain, frequently disrupting rest and causing nocturnal awakening.
The pain is often most severe during activities that create shear forces across the joint or require a single-leg stance.
- Stiffness After Rest
A period of immobility, such as prolonged sitting or sleep, often results in notable stiffness and pain upon the initial movements. This post-static stiffness occurs as the synovial fluid within the joint and the surrounding connective tissues become less pliable.
The first several steps after rising from a chair or getting out of bed in the morning are typically the most difficult and painful. This stiffness usually diminishes with gentle, progressive movement but reliably returns after another cycle of rest, forming a predictable pattern of discomfort.
The Surprising Ways the Pain Can Travel
The referral pattern of sacroiliac joint pain can complicate diagnosis, as it frequently mimics other common musculoskeletal and neurological conditions. This discomfort follows predictable pathways due to the shared nerve supply and biomechanical connections of the pelvic region, but it maintains distinguishing boundaries.
- Not Sciatica... But It Can Mimic It
A primary source of diagnostic confusion stems from the SI joint's ability to refer pain into the buttock and down the posterior thigh. This pattern arises from irritation of the lumbosacral nerve roots, which also innervate the joint itself, or from compensatory muscle spasms in the piriformis and gluteal regions.
The critical distinction lies in the nature and extent of the radiation. SI joint referral typically produces a deep, aching discomfort that rarely extends beyond the knee.
It generally lacks the sharp, electric, or burning quality of true radicular pain and is not associated with neurological deficits such as dermatomal numbness, specific muscle weakness, or loss of reflexes.
- Confusion with Hip Pain
Groin and lateral hip pain are common presentations of both SI joint dysfunction and primary hip pathology, such as osteoarthritis. The proximity of the anterior SI joint ligaments to the hip joint capsule, and the shared biomechanical role in weight-bearing, create this overlap.
A key differentiating factor is the location of maximal tenderness. Hip joint pathology typically elicits pain deep in the anterior groin, often worsened by internal rotation of the hip.
In contrast, SI joint pain centers posteriorly over the sacral sulcus, and its aggravating movements involve direct pelvic stress rather than isolated hip motion. Tests that load the SI joint without moving the hip, such as the FABER test, help clarify the source.
- Groin and Pelvic Discomfort
Referred pain can also manifest in the lower abdomen, groin, and even the upper lateral thigh due to irritation of the L2-L4 nerve roots that contribute to the SI joint's innervation. This pattern is particularly noted in cases of significant anterior SI ligament strain or inflammation.
- This discomfort is often described as a deep, vague ache rather than a sharp pain.
- It can be mistakenly attributed to visceral issues, sports hernias, or urological conditions, leading to unnecessary consultations and diagnostic tests.
- The presence of concurrent, more definitive posterior pelvic pain over the joint itself is the essential clue that points toward an SI joint origin for anterior symptoms.
Signs You Might Notice in Your Daily Movements
Beyond direct pain, sacroiliac joint dysfunction often presents with subtle, functional disturbances that manifest during routine activities. These signs reflect the joint's compromised role in providing a stable foundation for movement, leading to protective neuromuscular adaptations and a conscious avoidance of specific positions.
- Feeling "Unstable" or Like Your Leg Might Give Way
A common patient report is a subjective sensation of pelvic instability or a fear that the leg on the affected side will unexpectedly buckle during weight-bearing. This is not typically true muscular weakness detectable on manual muscle testing, but rather a proprioceptive disturbance and a neuromuscular guarding response.
The brain perceives instability in the core pelvic stabilizer, leading to a protective inhibition or altered firing pattern in the larger lower extremity muscles during dynamic tasks. Patients may describe a lack of trust in their stance on that side, especially when transitioning quickly or standing on uneven surfaces.
- Trouble Finding a Comfortable Position
Discomfort from SI joint stress is often posture-dependent, making sustained positions challenging. Patients frequently describe an inability to sit evenly, habitually shifting their weight off the painful side or perching on one buttock.
They may sit with their legs crossed in a specific pattern to unload the joint. In a supine position, lying flat on the back can sometimes increase lordotic stress on the joint, prompting individuals to place a pillow under their knees.
This constant postural adjustment is a direct effort to reduce compressive or shear forces on the inflamed articulation, and the search for relief becomes a persistent feature of daily life.
- Pain with Routine Transitions
Specific, often mundane, transitional movements become notable sources of pain due to the asymmetric loading they impose on the pelvis.
- Getting In and Out of a Car: This action requires a controlled, twisting transfer of weight with one leg fixed, placing direct rotational stress on the SI joint.
- Rolling Over in Bed: The uncoordinated, often reflexive motion of turning during sleep engages core and hip musculature that pulls on the pelvis, frequently jolting the joint and causing sharp pain that can awaken the individual.
- Bending Forward: Activities like tying shoes, washing one's face at a sink, or loading a dishwasher involve a forward flexion motion that can strain the posterior sacroiliac ligaments, especially when performed with the legs straight.
Best Sleeping Positions for Sacroiliac Joint Pain Relief
A precise diagnosis of sacroiliac joint dysfunction remains the essential prerequisite for effective long-term management, separating it from other spinal and pelvic pathologies. The unique pattern of localized pain and functional limitation directs targeted treatment strategies that address both joint inflammation and core instability.
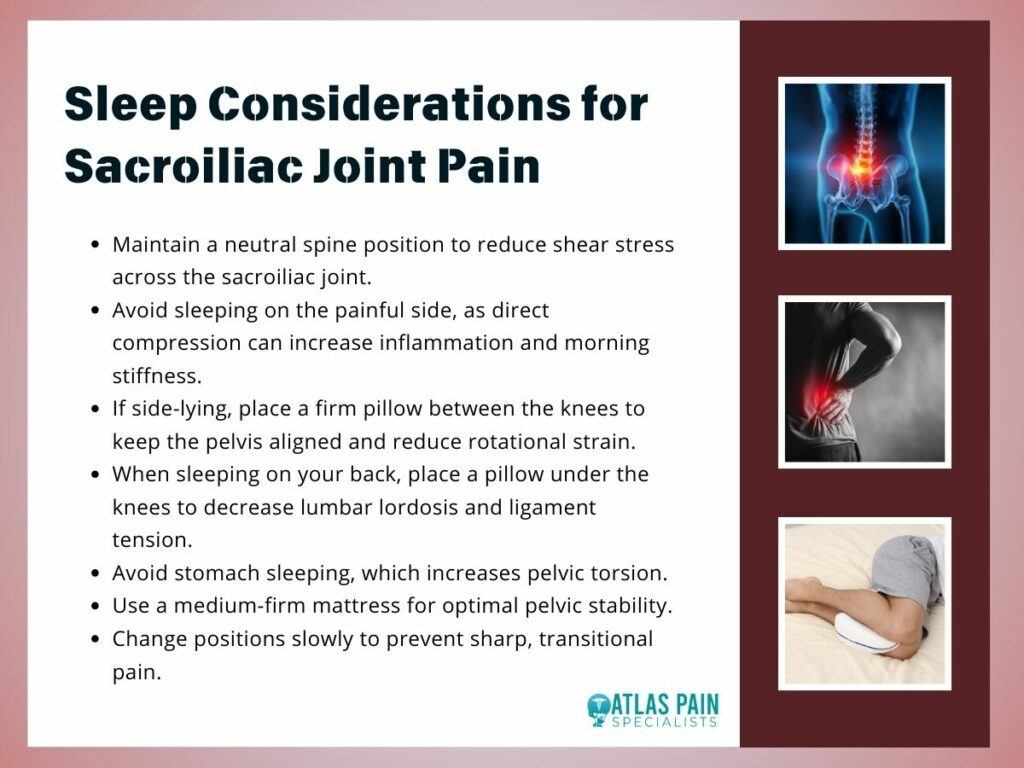
This specific symptom profile directly informs practical adjustments in daily life, particularly during extended periods of rest. For instance, sleeping on the painful side applies compressive force to the inflamed joint, and sleeping on the back with straight legs can increase lumbar lordosis, straining the sacroiliac ligaments.
Therefore, optimizing sleep posture becomes a critical component of conservative care, aiming to minimize nocturnal irritation. Positions that maintain neutral spinal alignment and reduce shear forces across the pelvis, such as side-lying with strategic pillow support between the knees or supine with a cushion under the legs, can help prevent morning stiffness and pain flare-ups.
Burning sensation in the leg below the knee is most commonly caused by nerve irritation, poor circulation, muscle strain, or underlying medical conditions, and it is relieved through proper diagnosis, targeted treatment, lifestyle changes, and supportive home care. This uncomfortable feeling may present as heat, tingling, or sharp pain and can range from mild and temporary to persistent and disruptive, depending on its underlying cause.
In this article, you will find a clear breakdown of the most common causes, associated symptoms, warning signs that require medical attention, diagnostic methods, and both medical and home-based relief options, along with practical prevention tips to help with burning sensation in leg below knee.
Common Causes of Burning Sensation Below the Knee

A burning sensation below the knee can arise from issues affecting nerves, muscles, blood flow, or the skin. Identifying the underlying cause is important to determine whether the problem is minor or requires medical attention.
1. Peripheral Neuropathy
Peripheral neuropathy occurs when the nerves that carry signals between the brain and legs are damaged. This can cause burning, tingling, numbness, or stabbing pain in the lower legs and feet. Common causes include diabetes, vitamin deficiencies, infections, and long-term alcohol use.
2. Sciatica
Sciatica results from compression or irritation of the sciatic nerve in the lower spine. It can cause burning or shooting pain that travels from the lower back down the thigh and below the knee. Pain often worsens when sitting, bending, or standing for long periods.
3. Nerve Entrapment Near the Knee
Nerves around the knee, particularly the peroneal nerve, may become trapped due to injury, swelling, or repetitive pressure. This can lead to burning, tingling, or weakness in the lower leg. Some people may also experience difficulty lifting the foot.
4. Poor Blood Circulation (Peripheral Artery Disease)
Narrowed arteries reduce blood flow to the legs, leading to burning, cramping, or aching, especially during walking or activity. Symptoms often ease with rest but return with movement.
5. Muscle Strain and Overuse
Overworking the lower leg muscles from running, long walks, or standing for extended periods can cause inflammation. This often results in a burning or aching sensation in the calf or shin. Rest, stretching, and proper footwear can help relieve discomfort.
6. Shin Splints
Shin splints occur when muscles, tendons, and tissues around the shinbone become inflamed due to repeated stress. This condition produces a burning, aching pain along the front or inner lower leg, especially during physical activity.
7. Skin Infections and Irritation
Skin infections like cellulitis, allergic reactions, or insect bites can cause redness, swelling, warmth, and a burning sensation below the knee. These conditions often require medical treatment, particularly if symptoms spread or are accompanied by fever.
Burning sensations below the knee can be minor or a sign of a more serious condition. Understanding the common causes helps guide appropriate treatment and ensures timely medical evaluation when necessary.
Symptoms That Often Accompany Burning Sensation
A burning sensation below the knee is often accompanied by other signs that help indicate its cause. Recognizing these symptoms can guide proper treatment and care.
- Tingling or “pins and needles” - Feels like small pricks or buzzing under the skin, often linked to nerve irritation.
- Numbness or reduced sensation - The leg may feel dull or less sensitive, sometimes affecting balance.
- Sharp or shooting pain - Sudden, intense pain that may radiate down the leg, often related to nerve issues.
- Swelling in the lower leg - The leg may appear puffy or tight, usually from inflammation, poor circulation, or injury.
- Redness or warmth of the skin - Indicates irritation, infection, or increased blood flow, often intensifying the burning sensation.
- Muscle weakness or fatigue - Weakness may occur when nerves or muscles are affected, making walking or standing difficult.
Burning sensations below the knee are often accompanied by symptoms like tingling, numbness, pain, swelling, or skin changes. Noting these signs can help identify the underlying cause and guide timely treatment.
When to See a Doctor (Urgent Red Flags)

While a burning sensation below the knee is often mild and temporary, certain warning signs may indicate a serious underlying problem. If any of the following symptoms appear, prompt medical attention is important.
1. Sudden or severe leg pain
Intense or unexpected pain may signal nerve injury, blood clots, or circulation problems. This type of pain should not be ignored, especially if it worsens quickly.
2. Swelling, warmth, or redness in the leg
These symptoms can point to infection or a possible blood clot in the leg. Immediate medical evaluation is needed to prevent complications.
3. Loss of sensation or muscle weakness
Numbness or weakness may indicate nerve damage or spinal issues affecting the leg. If left untreated, this can lead to long-term mobility problems.
4. Fever or signs of infection
Fever combined with leg pain or redness may indicate a serious infection spreading through the tissues. Medical care is necessary to control the infection and avoid further harm.
5. Chest pain or shortness of breath
These symptoms can occur if a blood clot travels to the lungs, which is a life-threatening emergency. Seek urgent medical help right away.
Although many cases of burning sensation in the leg are not dangerous, the presence of these red flags should never be ignored. Recognizing and acting on these warning signs can help prevent serious health complications and ensure timely treatment.
Diagnosing the Cause
To determine what is causing a burning sensation below the knee, doctors use a combination of medical history, physical examination, and diagnostic tests. These tools help identify whether the issue is related to nerves, circulation, muscles, or an underlying medical condition.
1. Medical history and physical exam
The doctor will ask about symptoms, lifestyle, and existing health conditions while checking strength, reflexes, and areas of tenderness. This helps narrow down the most likely source of the problem.
2. Blood tests
Blood work can detect conditions such as diabetes, vitamin deficiencies, inflammation, or infection. These results help identify systemic causes that may affect nerve or muscle health.
3. Nerve conduction studies
These tests measure how well electrical signals travel through the nerves. They are useful for diagnosing nerve damage or compression.
4. Imaging tests (X-ray, MRI, or CT scan)
Imaging allows doctors to see bones, muscles, and nerves to detect injuries, disc problems, or structural abnormalities. These scans are especially helpful if nerve or spinal issues are suspected.
5. Vascular tests (ultrasound or Doppler studies)
These tests evaluate blood flow in the legs and help detect narrowed arteries or blood clots. They are essential when circulation problems are suspected.
Accurate diagnosis is key to effectively treating a burning sensation below the knee. By using a combination of exams and tests, healthcare providers can pinpoint the underlying cause and recommend the most appropriate treatment.
Relief & Treatment Strategies

Relieving a burning sensation below the knee depends on identifying and addressing its underlying cause. A combination of home care, medical treatment, and lifestyle adjustments can help reduce discomfort and promote healing.
1. Rest and Activity Modification
Resting the affected leg helps reduce inflammation and prevent further strain on muscles and nerves. Avoid activities that worsen the burning sensation, and gradually resume movement to prevent recurrence.
2. Ice and Heat Therapy
Ice can numb pain and reduce swelling after injury or overuse, while heat relaxes tight muscles and improves blood flow. Using the right method for your symptoms can relieve discomfort effectively.
3. Medications
Over-the-counter pain relievers and anti-inflammatories can help control pain and swelling. For nerve-related burning, doctors may prescribe specific medications to calm nerve pain, always under professional guidance.
4. Physical Therapy
Therapy strengthens muscles, improves flexibility, and reduces pressure on irritated nerves. Stretching and posture techniques taught by a therapist can promote long-term relief and prevent symptoms from returning.
5. Treating Underlying Medical Conditions
Addressing conditions like diabetes, vitamin deficiencies, or circulation problems is key for lasting relief. Treating the root cause prevents further nerve or tissue damage rather than just relieving symptoms temporarily.
6. Compression and Support
Compression socks or supportive braces improve circulation, reduce swelling, and provide stability. They are especially useful for those who spend long periods standing or walking.
Effective relief for a burning sensation below the knee usually combines self-care, medical treatment, and lifestyle adjustments. Treating the root cause while managing symptoms helps speed recovery and maintain long-term comfort.
Preventing Recurrence
Preventing a burning sensation below the knee involves maintaining healthy nerves, muscles, and circulation. Simple lifestyle and self-care habits can greatly reduce the risk of symptoms returning.
1. Manage blood sugar levels
Keeping blood sugar under control helps protect nerves from damage, especially for people with diabetes. This can significantly lower the risk of burning and tingling sensations.
2. Stay physically active
Regular exercise improves circulation and strengthens the muscles that support the legs. Gentle activities such as walking and stretching help keep tissues healthy and flexible.
3. Use proper footwear
Wearing well-fitted, supportive shoes reduces strain on the lower legs and improves posture and balance. This can help prevent muscle fatigue and nerve compression.
4. Avoid prolonged pressure on the legs
Sitting or standing in one position for too long can restrict blood flow and irritate nerves. Changing positions regularly helps maintain healthy circulation.
5. Maintain a healthy weight
Excess weight increases pressure on the legs, joints, and nerves. Maintaining a healthy weight reduces strain and lowers the risk of recurring symptoms.
Taking preventive steps can make a major difference in keeping burning leg sensations from returning. By supporting overall leg health and addressing risk factors, you can enjoy greater comfort and long-term mobility.
When Burning Sensation Is Harmless vs. Concerning
Not all burning sensations below the knee are a cause for alarm. Understanding the difference between harmless discomfort and symptoms that may indicate a serious underlying condition can help you decide when to seek medical attention.
| Feature | More Likely Harmless | More Concerning |
| Timing | Mild burning after exercise or standing long periods | Persistent or worsening burning without a clear trigger |
| Pain Level | Slight discomfort that eases with rest | Severe or sudden pain that does not improve |
| Associated Symptoms | Minimal or none; may include mild fatigue | Swelling, redness, warmth, numbness, weakness, or fever |
| Response to Home Care | Improves with rest, stretching, or ice/heat | Does not improve with basic care and continues to interfere with daily activities |
| Pattern | Occasional or short-lived | Progressive or spreading over time |
A burning sensation below the knee is usually harmless after exercise or minor strain, but persistent, severe, or worsening symptoms—especially with swelling, numbness, or skin changes—require prompt medical evaluation to prevent complications.
Wrapping Up
A burning sensation below the knee can result from nerves, circulation issues, muscle strain, or underlying medical conditions. While mild, occasional discomfort is often harmless, persistent or severe symptoms especially with swelling, numbness, or redness require medical evaluation.
Managing this condition involves proper diagnosis, targeted treatment, and lifestyle measures. Combining home care, preventive habits, and timely medical attention can relieve symptoms, prevent recurrence, and help maintain healthy, pain-free legs.
Back pain can be frustrating when every test seems to say “normal.” Sometimes, even advanced imaging like MRI or CT scans fail to reveal the exact source of pain. In these cases, a special diagnostic procedure called a discogram can help.
So, what Is a discogram and when is it needed? A discogram, or discography, is a test doctors use to determine whether a specific spinal disc is causing pain.
It goes beyond simple imaging by recreating the pain in a controlled way to confirm the true source. This article explores how discograms work, when they are used, what patients can expect, and what happens after the test.
Understanding How a Discogram Works
A discogram is not a typical imaging test. It combines imaging with a pain-provocation technique that targets spinal discs suspected of causing chronic back pain. During the procedure, a radiologist or spine specialist injects a contrast dye into one or more discs under X-ray guidance.
The injected dye highlights the disc on imaging and can also reproduce the patient’s usual pain.The most important thing to know is that a discogram helps identify which disc is truly causing pain rather than just showing structural abnormalities.
Many people have bulging or worn discs that do not cause any discomfort. The discogram distinguishes between “painful” and “non-painful” discs, allowing doctors to plan effective treatment.
The Anatomy Behind the Test
Between each vertebra in the spine sits a cushion-like structure called an intervertebral disc. These discs act as shock absorbers and allow flexibility.
Each disc has a tough outer layer, the annulus fibrosus, and a soft inner core, the nucleus pulposus. Over time or after injury, discs can degenerate or tear, sometimes leading to chronic low back or neck pain.
A discogram targets these discs one by one. When contrast dye is injected, it increases pressure inside the disc. If that disc is healthy, the patient may feel only mild pressure.
But if the disc is damaged, the dye may leak through small tears, producing pain that matches the patient’s everyday symptoms. This match is what makes the test valuable.
The Procedure Step by Step

- Preparation: The patient lies on a table in a sterile procedure room, usually in a hospital or outpatient radiology center. An intravenous line delivers medication to relax the body but not put the patient fully to sleep.
- Numbing the Area: The doctor cleans and numbs the skin and tissues over the spine using local anesthesia.
- Needle Placement: Using fluoroscopy, a type of live X-ray, the physician guides thin needles into the target discs.
- Contrast Injection: A small amount of contrast dye is injected into each disc. The doctor asks the patient to describe sensations in real time, noting whether the injection reproduces their typical pain.
- Imaging: X-ray or CT images are taken immediately afterward to visualize the shape and integrity of the discs and the spread of contrast dye.
The entire procedure usually takes 30 to 60 minutes. Patients go home the same day after a short recovery period.
When Doctors Recommend a Discogram
Discograms are not for everyone with back pain. They are typically recommended only after conservative treatments and standard imaging fail to explain ongoing pain. Physicians consider several criteria before ordering one.
A discogram is often used when surgical decisions depend on pinpointing which disc is the real problem. For example, if an MRI shows multiple degenerated discs, a discogram can clarify which one is symptomatic so that surgery or targeted therapy focuses on the correct area.
Common Situations That Lead to a Discogram
- Persistent back or neck pain lasting more than three months despite physical therapy, medications, or injections
- Inconclusive MRI or CT scans that show changes but cannot explain the symptoms
- Planning for spinal fusion or artificial disc replacement where identifying the correct disc is crucial
- Evaluating post-surgical pain to determine if pain comes from a previously treated disc or another level
The goal is always to obtain precise information before performing irreversible treatments. The test can prevent unnecessary surgery by confirming that certain discs are not painful at all.
Who Should Avoid a Discogram
Certain conditions make the test inappropriate or risky. Doctors typically avoid discography in patients with active infections, severe allergies to contrast dye, bleeding disorders, or pregnancy.
People with primarily nerve-related pain, such as sciatica from a herniated disc pressing on a nerve, usually do not benefit from a discogram because the test targets disc pain, not nerve compression.
Benefits and Limitations of Discography

Like any medical test, a discogram has both strengths and weaknesses. Understanding them helps patients make informed decisions.
Key Benefits
Discograms can reveal pain sources that imaging alone cannot identify. MRIs show structure, but they cannot always tell whether a visible disc abnormality causes pain.
By comparing pain responses across multiple discs, doctors get functional information that guides treatment. Another advantage is surgical planning accuracy.
A 2020 study in The Spine Journal found that patients who had discograms before spinal fusion were more likely to have successful outcomes because surgeons could better target the pain-producing discs.
The test can also help rule out surgery if no painful disc is found, preventing unnecessary operations.Discograms offer psychological reassurance to patients.
Knowing exactly which disc is problematic and that the pain is real and identifiable can help reduce uncertainty and anxiety. It provides a tangible explanation for chronic pain that may have persisted for years without answers.
Limitations to Consider
However, discograms are not perfect. The procedure can temporarily increase back pain, and results depend on the patient’s pain descriptions, which introduces subjectivity. In rare cases, the injected dye can irritate or inflame a disc, causing discomfort for a few days.
Some experts also question whether discography always predicts surgical success. A 2019 American Journal of Neuroradiology review noted that pain reproduction is helpful but not infallible. Disc degeneration often exists in several levels, and distinguishing which one is most responsible for pain can be challenging.
| Aspect | Strengths | Limitations |
| Purpose | Identifies pain-producing discs | May not detect nerve-related pain |
| Accuracy | More specific than MRI alone | Dependent on patient pain feedback |
| Imaging | Combines fluoroscopy and CT for detail | Dye injection can cause short-term pain |
| Outcome Use | Guides targeted surgery or therapy | Cannot always predict long-term results |
| Recovery | Usually same-day discharge | Mild soreness possible for a few days |
Overall, when used for the right reasons, a discogram remains a valuable diagnostic option in complex spine cases.
What Patients Can Expect After the Procedure
After the discogram, patients rest in a recovery area for about 30 to 60 minutes. The doctor monitors vital signs and ensures pain levels are manageable. Mild soreness at the injection site or temporary worsening of back pain is common but usually fades within a few days.
Following the procedure, patients are advised to rest and avoid heavy lifting or strenuous activity for 24 hours. Ice packs and over-the-counter pain medicine often provide relief. Most people return to normal activities the next day, though doctors may recommend waiting longer if discomfort persists.
The Role of Post-Discogram CT Scans
Many clinics perform a CT scan immediately after the discogram while the dye is still visible. The CT shows detailed cross-sections of each disc, allowing doctors to see internal tears or leaks where contrast has escaped. This combined information the pain response and the imaging pattern offers a complete diagnostic picture.
Understanding Results
Doctors interpret the findings based on three main factors:
- Pain Response: If a particular disc reproduces the patient’s usual pain, it is considered “positive.”
- Imaging Findings: CT scans reveal whether dye spread indicates tears, fissures, or degeneration.
- Comparison with Other Discs: Healthy discs serve as controls. A positive response in one disc but not others strengthens the diagnosis.
Within a few days, the physician reviews the results with the patient. Together they discuss next steps, which might include continued non-surgical management or surgical consultation.
Long-Term Follow-Up
Some patients experience temporary relief after the injection, while others notice increased pain for a few days. This does not necessarily mean the discogram worsened their condition it simply reflects the disc’s sensitivity.
Most people return to their pre-test baseline within a week. Doctors may schedule follow-up appointments to assess pain patterns and discuss treatment options such as physical therapy, epidural injections, or surgery.
Risks, Safety, and Evolving Techniques
Although discograms are generally safe, they are invasive, and every procedure carries some risk. The overall complication rate is low, but awareness helps patients prepare realistically.
Potential Risks
- Infection: Very rare (less than 1% according to a 2022 Radiology report) but possible if bacteria enter the disc during needle insertion.
- Bleeding or nerve irritation: Uncommon, typically mild and temporary.
- Disc damage: Repeated injections or improper technique can, in theory, weaken a disc, though this is rare with modern sterile practices.
- Allergic reaction: Some people may react to the contrast dye, though pre-screening and test doses minimize this risk.
To minimize risk, doctors use strict sterile techniques, fluoroscopic guidance, and single-use needles. Most complications are minor and resolve quickly.
Advances in Discography Technology
Recent innovations have made the test more precise and comfortable. Digital pressure sensors now measure the exact amount of force applied during dye injection, allowing better correlation between pressure and pain.
Some centers use low-volume dye techniques to reduce irritation. In addition, high-resolution CT and MRI follow-ups provide clearer visualization of internal disc structure.
These advances are helping discography remain relevant in the era of high-tech imaging, ensuring it continues to offer unique insights into spine pain.
Alternatives to Discography
If a doctor decides a discogram is not appropriate, other diagnostic tools may be considered. These include:
- MRI with contrast, which highlights inflammation around nerves or discs.
- Facet joint injections, used to identify pain from joints rather than discs.
- Nerve blocks, which temporarily numb specific spinal nerves to see if pain decreases.
Each test serves a different purpose, and sometimes they are used together to form a complete diagnostic picture. Combining results allows physicians to customize care for each patient, ensuring that treatment addresses the true cause of pain.
What Is a Discogram: Understanding Its Role in Future Back Care
Discograms are a bridge between imaging and experience they connect what doctors see with what patients feel. By recreating pain under controlled conditions, the test clarifies which spinal discs are truly responsible for chronic discomfort. It is not the first step in diagnosis, but it becomes essential when pain remains unexplained after standard tests.
Discograms continue to be a key link between traditional radiology and modern surgical planning, providing precision that many other tests lack. As spine care continues to evolve, discography’s role may shift toward integration with advanced imaging and regenerative medicine.
For patients, this means more personalized care and fewer unnecessary surgeries. Discography results could help guide new treatments like stem cell injections or minimally invasive disc repair techniques. These emerging therapies depend on accurate mapping of the pain source something discograms are uniquely designed to provide.
An epidural steroid injection is a common procedure used to provide relief from pain caused by issues such as herniated discs, sciatica, spinal stenosis, and other spine-related conditions. This injection delivers steroids directly into the epidural space around the spinal cord and nerve roots, reducing inflammation and alleviating pain. While the procedure can be highly effective, recovery is an important process, and sleeping positions play a significant role in your comfort and healing.
In this article, we will discuss the best position to sleep after an epidural steroid injection, the benefits of each position, and the overall impact of proper rest on your recovery. We’ll also explore how specific sleeping positions can help with other types of pain, such as sacroiliac joint pain, which is common after certain spinal procedures.
Understanding Epidural Steroid Injections and the Importance of Recovery
An epidural steroid injection can be a game-changer for patients experiencing debilitating back or leg pain. Whether due to a herniated disc, spinal stenosis, or other conditions, these injections help reduce inflammation, alleviate pain, and improve mobility. However, proper recovery after the injection is just as important as the procedure itself.
One of the most critical aspects of recovery is ensuring that you sleep in a position that does not place unnecessary strain on the injection site. The right sleeping position can promote healing, reduce discomfort, and support your overall recovery process. Poor sleep positioning, on the other hand, can lead to prolonged pain, discomfort, and even further injury.
General Sleep Guidelines After an Epidural Steroid Injection
When recovering from an epidural steroid injection, the main goal is to ensure that the area of the spine or the nerves targeted by the injection is properly supported while you sleep. Doctors often recommend staying in a position that keeps your spine aligned and reduces pressure on the lower back, particularly around the area where the injection was administered. Additionally, you may need to make use of pillows or other supports to keep your body in the correct posture and avoid strain.
Good sleep hygiene is important. You should also avoid twisting, bending, or moving abruptly, as these actions can exacerbate pain or cause injury.
Best Sleeping Positions After the Procedure
The following positions are generally considered the best for sleeping after an epidural steroid injection:
1. Sleeping on Your Back
Sleeping on your back is considered the most recommended position after an epidural steroid injection. This position helps to maintain a neutral spine, which minimizes pressure on the injection site. When you lie on your back, your weight is evenly distributed across the mattress, which helps reduce stress on your spine and lower back muscles.
Benefits:
- Reduces pressure on the spine: When lying flat on your back, your spine stays in a neutral position, allowing for even distribution of weight across the mattress. This can help prevent unnecessary pressure on the spinal discs, nerves, and muscles.
- Eases discomfort: The position can provide relief from discomfort by keeping your body aligned. This helps reduce the likelihood of developing stiffness, soreness, or muscle spasms after the procedure.
- Supports proper posture: Lying on your back with proper support (e.g., using pillows) ensures that your neck, spine, and lower back stay in alignment, which promotes healing and recovery.
How to sleep in this position:
- Place a small pillow or cushion under your knees to help relieve tension in the lower back and support the natural curve of your spine.
- Use a supportive pillow under your head to ensure that your neck stays in a neutral position and does not get strained.
- If needed, a rolled towel or lumbar cushion placed under the small of your back can offer additional support.
2. Sleeping on Your Side
Sleeping on your side is another comfortable and beneficial position after an epidural steroid injection, especially if you find it difficult to sleep on your back. This position can reduce pressure on the spine while allowing you to maintain a relatively neutral posture.
Benefits:
- Less pressure on the spine: Sleeping on your side can reduce pressure on the spine and injection site, particularly if you use pillows for support.
- Comfortable for those with sacroiliac joint pain: This position can also help alleviate sacroiliac joint pain (discomfort in the pelvic area), which often occurs after spinal procedures. It provides better distribution of weight to minimize strain.
- Improved circulation: By sleeping on your side, you can prevent restricted blood flow to certain parts of your body, especially if you use a pillow between your legs for added comfort.
How to sleep in this position:
- Place a firm pillow between your knees to keep your hips aligned and reduce strain on your lower back.
- Ensure that your neck and spine stay aligned by using a pillow that supports the natural curve of your neck.
- If you feel any discomfort, experiment with the height and thickness of the pillow to find the best position for your body.
3. Avoid Sleeping on Your Stomach
Although some people may be accustomed to sleeping on their stomach, this is generally not recommended after an epidural steroid injection. Sleeping on your stomach can place significant pressure on the neck and lower back, which can disrupt the healing process.
Why stomach sleeping is not recommended:
- Strains the spine and neck: Sleeping on your stomach can cause your spine to remain in an unnatural position, leading to discomfort and muscle strain. It can also strain your neck because you’ll likely have to turn your head to one side to breathe.
- Increases pressure on the injection site: If the injection was administered in the lower back or spinal area, stomach sleeping can increase pressure on the spinal discs, making it harder for the area to heal.
- Hinders proper alignment: This position may misalign your body, causing further discomfort in the lower back, hips, and shoulders.
To avoid stomach sleeping, consider using body pillows or other supports to help train your body to stay on the side or back sleeping positions throughout the night.
Supporting Your Body for Comfort
Even if you are sleeping on your back or side, the use of additional pillows or cushions can greatly enhance your comfort and support. Here are a few tips for supporting your body:
1. Using Pillows for Lumbar Support
A pillow or cushion placed under your knees when lying on your back can help maintain the natural curve of your lower back and reduce pressure on the spinal discs. This is especially important if you have had an epidural injection in the lower back area.
When sleeping on your side, using a pillow between your knees helps align your hips and lower back, preventing torsion and strain. Make sure the pillow is thick enough to keep your hips properly aligned and your spine in a neutral position.
2. Elevating Your Legs
Elevating your legs can help reduce pressure on the lower back and encourage better circulation throughout your body. This position can be especially helpful if you have sciatica or sacroiliac joint pain, as it reduces the strain on the affected areas.
By elevating your legs with a cushion or pillow while sleeping on your back or side, you allow your spine and hips to rest in a more natural, neutral position, which promotes faster recovery. This simple adjustment can make a significant difference in reducing discomfort and improving your overall sleep quality. Try adjusting the height of your pillows for the best comfort and support.
3. Mattress and Bed Adjustments
The type of mattress you sleep on can also impact your comfort. A medium-firm mattress is typically recommended for people recovering from an epidural steroid injection, as it provides a balance of support and softness. You may also want to consider using a memory foam mattress topper for extra comfort and to reduce pressure points.
Post-Procedure Tips for a Better Sleep Experience
While sleeping positions are crucial for recovery, there are additional tips that can help improve your sleep quality and support the healing process after an epidural steroid injection:
- Gentle stretching: Before going to bed, perform some gentle stretches to help relax your muscles and relieve any tension. However, avoid vigorous stretching or exercises that could strain the injection site.
- Move cautiously: Be mindful of your movements when you wake up. Sudden movements or twisting can aggravate the injection site. Try to slowly roll to one side and use your arms to push yourself into a seated position.
- Sleep on your back for the first few days: If you’re unsure about the best sleeping position, sticking to back sleeping for the first few nights can give your body time to adjust. Once you feel more comfortable, you can experiment with side sleeping.
Conclusion: Best Sleeping Positions for Sacroiliac Joint Pain Relief
When dealing with sacroiliac joint pain, sleeping positions like lying on your back with proper support or sleeping on your side with a pillow between your legs can offer significant relief. These positions ensure comfort while minimizing strain on the lower back and pelvic area, helping with overall recovery after both epidural injections and sacroiliac joint discomfort.
In conclusion, the best position to sleep after an epidural steroid injection is one that supports proper spinal alignment, reduces pressure on the injection site, and provides comfort. Whether you choose to sleep on your back or side, using pillows for additional support and avoiding stomach sleeping can help facilitate a smoother recovery process.
Be mindful of your movements, use proper sleep hygiene, and consult with your healthcare provider to ensure that you are following the most suitable recovery plan for your individual needs. Resting properly and following these sleeping guidelines can significantly enhance your recovery and overall well-being during the healing process.
Living with chronic nerve pain can affect how you move, sleep, and manage daily responsibilities, including caring for your home and family. When pain becomes constant, knowing your treatment options becomes part of protecting your quality of life and long-term well-being.
You may have heard about different nerve stimulation options and felt unsure about what actually separates one from another. Confusion often comes from treatments being grouped together, even though they work in very different ways and target pain at different points in the nervous system.
Many people assume nerve stimulation treatments are either experimental or meant only as a last resort, which leads to confusion and hesitation. Others believe all stimulation therapies work the same way, without realizing how much precision can matter for certain types of pain. Let's look at how the dorsal root ganglion stimulation procedure.
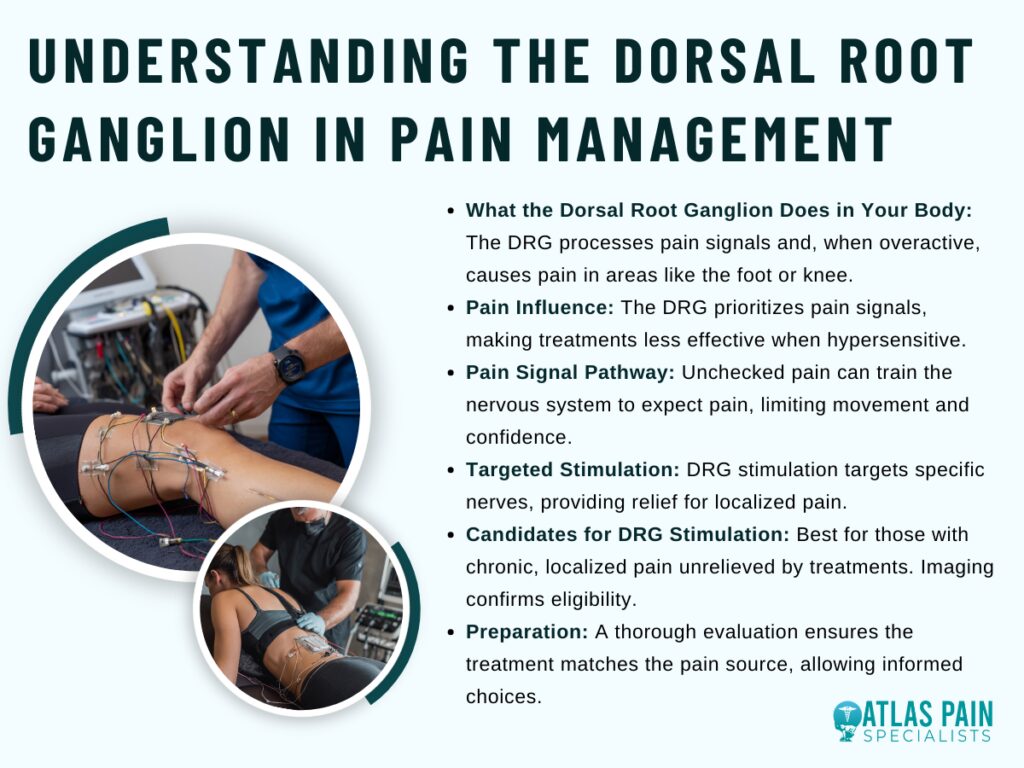
- What the dorsal root ganglion does in your body
Your nervous system controls how pain reaches your brain, even when the source feels small or localized. When pain lingers or feels out of proportion, the issue often lies in how those signals travel rather than where they start.
This part of the body rarely gets attention because you cannot see or feel it directly. Still, it plays a major role in why certain pain stays sharp, focused, and difficult to manage with common treatments.
What the dorsal root ganglion actually is
The dorsal root ganglion is a small cluster of nerve cells located just outside the spinal cord. It acts as a checkpoint where sensory information, including pain, enters the central nervous system.
Because many pain signals pass through this area, even minor disruption here can change how strongly pain registers. When this checkpoint stays overactive, pain can feel constant or exaggerated.
Why it influences pain more than other nerve areas
This structure handles very specific sensory input from defined parts of your body. That specificity means pain does not spread randomly but stays locked into certain regions like a foot, knee, or groin.
When the dorsal root ganglion becomes hypersensitive, those signals gain priority over others. Ignoring this mechanism often leads to treatments that dull sensation broadly but never fully address the source.
What happens when pain signals pass through unchecked
Pain signals that move freely through this area reach the brain without interruption. Over time, that steady input can train your nervous system to expect pain even during normal movement.
This response can limit mobility and confidence, even when tissue damage remains minimal. Addressing the signal pathway itself can reduce that cycle instead of masking it.
- Why this therapy is different from other nerve pain treatments
Different types of nerve pain respond differently to different treatments, and that can feel frustrating when options start to blur together. Targeted approaches exist because broad solutions often leave certain pain patterns untouched.
You may have tried treatments that helped briefly or reduced pain in some areas but not others. This difference usually comes down to how precisely the therapy interacts with the nerve pathways involved.
How targeted stimulation changes the approach
This therapy focuses on influencing pain signals at a very specific entry point into the nervous system. Instead of affecting wide regions of the spine, it concentrates on the exact nerves responsible for your pain.
That focus allows relief without numbing surrounding areas. When pain stays localized, precision often matters more than strength.
How it compares to traditional spinal cord stimulation
Traditional spinal cord stimulation works by covering larger nerve regions to reduce pain perception. While that method helps many people, it can struggle with pain that remains sharp and confined.
This therapy offers more control over where stimulation occurs. Without that control, certain pain patterns continue despite multiple adjustments.
Why precision can lead to more consistent relief
Precise placement allows stimulation to stay aligned with your pain even as you move. That consistency can reduce the ups and downs often felt with broader treatments.
When therapy shifts with posture or activity, relief becomes unpredictable. Addressing the signal at its source can create steadier results over time.
- Who may be a good candidate for DRG stimulation
Chronic pain does not follow one pattern, which makes choosing the right treatment feel overwhelming. Some approaches work best when pain stays focused in one area rather than spreading or changing day to day.
Knowing who this therapy tends to help can save time, cost, and frustration. It also allows you to have a more productive conversation with a specialist instead of trying options through trial and error.
Pain types that often respond well to this therapy
This therapy commonly helps pain that stays confined to a specific region of the body. Conditions involving nerve injury or nerve sensitivity in areas like the foot, knee, groin, or lower leg often fit this profile.
Because the pain remains localized, targeted stimulation can address it directly. Treating this kind of pain with broad methods can leave relief incomplete.
When other treatments have not provided lasting relief
Many candidates reach this option after medications, injections, or physical therapy fail to provide consistent improvement. Temporary relief often signals that the pain pathway itself remains active.
This therapy addresses that pathway rather than symptoms alone. Continuing the same treatments despite limited results can delay meaningful progress.
Health and evaluation factors that influence eligibility
Your overall health, prior procedures, and pain history play a role in determining suitability. Imaging and nerve mapping help confirm whether the pain pathway aligns with this approach.
Careful evaluation reduces the risk of unnecessary procedures. Skipping this step can lead to treatment that never fully matches your condition.
- What happens before the procedure
Preparing for this procedure involves more than scheduling a date and showing up. The steps beforehand shape how effective the therapy can be and help avoid surprises later.
Taking time to evaluate your pain and your goals allows the care team to tailor the approach to you. This phase also gives you space to ask questions and decide with confidence rather than pressure.
How your pain is evaluated and mapped
Your provider reviews where your pain starts, how it feels, and what makes it better or worse. Imaging and nerve assessments help connect your symptoms to specific nerve pathways.
This process clarifies whether the pain aligns with the area this therapy targets. Skipping detailed evaluation can lead to treatment that misses the true source.
Why a trial stimulation is part of the process
A trial allows you to experience the therapy before committing to a permanent device. Temporary leads test how well targeted stimulation reduces your pain during normal activity.
This step helps confirm benefit in real-life conditions rather than theory. Moving forward without a trial increases uncertainty about results.
Planning and preparation before the implant
Once the trial shows improvement, planning focuses on lead placement and device positioning. Instructions before the procedure help reduce infection risk and support smoother recovery.
Clear preparation also sets expectations for activity and follow-up. Poor planning often leads to unnecessary delays or complications.
- What happens before the procedure
Before anything physical takes place, the focus stays on clarity and alignment. This stage exists to make sure the treatment fits your pain pattern and your expectations, not just a diagnosis on paper.
Time spent preparing often determines how confident you feel moving forward. It also reduces the chance of pursuing a solution that does not truly match what your body needs.
How your pain story gets carefully reviewed
Your provider starts by listening to how your pain shows up in daily life, not just where it hurts. Details like consistency, triggers, and past treatments help narrow the nerve pathway involved.
Imaging and clinical findings then support that picture. Without this level of review, treatment can aim at the wrong target.
Why a trial phase comes before anything permanent
The trial phase gives you firsthand experience with how targeted stimulation affects your pain. Temporary leads allow you to test relief during normal movement and routine activities.
This step confirms real-world benefit rather than relying on assumptions. Skipping a trial increases the risk of committing to something that feels right in theory but not in practice.
How planning and preparation shape the outcome
Once the trial shows meaningful improvement, planning becomes more specific. Placement strategy, timing, and pre-procedure instructions all factor into how smoothly things progress.
Proper preparation supports comfort and reduces avoidable complications. Rushing this phase can limit the long-term success of the therapy.
- Step by step look at the DRG stimulation procedure
Going into the procedure can feel intimidating if you only picture surgery or hospital visits. Knowing the steps beforehand can help you feel more in control and prepared for what actually happens.
The procedure itself is designed to be precise while minimizing disruption to your daily life.
How the procedure begins and what to expect
You arrive at the facility after following pre-procedure instructions, such as fasting or adjusting medications. Sedation or local anesthesia helps you stay comfortable while remaining aware enough to respond if needed.
The team ensures the environment is sterile and that monitoring is in place. Attention to these details keeps the process safe and focused.
Placement of the leads and device
Leads are carefully guided to the area near the dorsal root ganglion where pain signals enter the nervous system. Imaging tools confirm the precise location, and adjustments happen as needed.
Once the leads sit correctly, the device is positioned and secured. Accurate placement is crucial for consistent pain relief.
Testing and final adjustments during the procedure
After placement, stimulation is tested to confirm that the targeted area responds as expected. Minor adjustments can be made on the spot to optimize relief.
The team observes your response closely before completing the procedure. Taking this step seriously improves the chances of long-term success.
- How the stimulation actually reduces pain
The therapy works by interrupting the way pain signals travel from your body to your brain. Instead of affecting large areas, it focuses on the specific nerves causing the discomfort, which can make relief more precise and consistent.
This targeted approach allows you to regain control over movements that previously triggered sharp or persistent pain. By managing the signals before they reach your brain, daily activities can feel less limited and more predictable.
How electrical signals interact with the dorsal root ganglion
Leads deliver mild electrical pulses directly to the nerve cluster responsible for your pain. These pulses adjust how the nerves communicate, reducing the intensity of the signals that reach your brain.
When the signals are tempered, you experience less discomfort during everyday motion. Ignoring this mechanism can leave traditional therapies less effective.
Why targeting a specific nerve cluster matters
Pain often follows predictable paths along certain nerves, and the dorsal root ganglion handles input from a defined area of your body. By focusing stimulation on this cluster, relief can stay localized rather than affecting unrelated regions.
This precision matters for chronic or sharp pain that does not respond well to broader therapies. Without targeted intervention, pain may continue despite multiple treatment attempts.
How consistent stimulation supports long-term relief
Keeping the stimulation aligned with the affected nerves allows pain control to remain steady over time. Adjustments can be made to match changes in activity or posture, maintaining effectiveness throughout the day.
This steady control helps prevent sudden flare-ups and supports more predictable daily function. Neglecting regular adjustments can reduce the therapy’s benefit.
What is Spinal Cord Stimulation and How Can It Relieve Pain?
Dorsal root ganglion stimulation can give you more confidence in managing chronic nerve pain. This therapy focuses on the precise pathways where pain signals travel, which often makes relief more targeted and consistent than broader approaches.
Spinal cord stimulation relates closely to this process because it also targets nerve signals to reduce pain, but it works over a broader area rather than focusing on a single nerve cluster. By comparing the two, you can see how the choice of therapy depends on the type and location of your pain.
Thinking about how targeted nerve therapies function connects directly to practical outcomes, like improving your ability to perform everyday tasks without constant discomfort. When you understand the mechanisms behind both dorsal root ganglion and spinal cord stimulation, you can communicate more effectively with your provider and track your progress.