New Location at 8406 E. Shea Blvd #100, Scottsdale 85260 - Accepting New Patients
Stellate Ganglion Blocks Explained: What to Expect and How They Work
Date: April 27, 2026
A stellate ganglion block injects local anesthetic near a nerve bundle in the lower neck. This procedure temporarily interrupts overactive sympathetic signals that drive chronic pain, post-traumatic stress, and long COVID symptoms.
The stellate ganglion sits along the spinal column and acts as a relay station for fight-or-flight responses. When this nerve cluster fires too aggressively, it can cause persistent arm pain, insomnia, and a racing heart.
One injection often produces immediate warmth and redness in the affected hand. That physical sign confirms the block successfully relaxed the nerve's grip on blood vessels and sweat glands. Let's look at stellate ganglion blocks explained , what to expect and how they work.
What Is a Stellate Ganglion Ganglion?
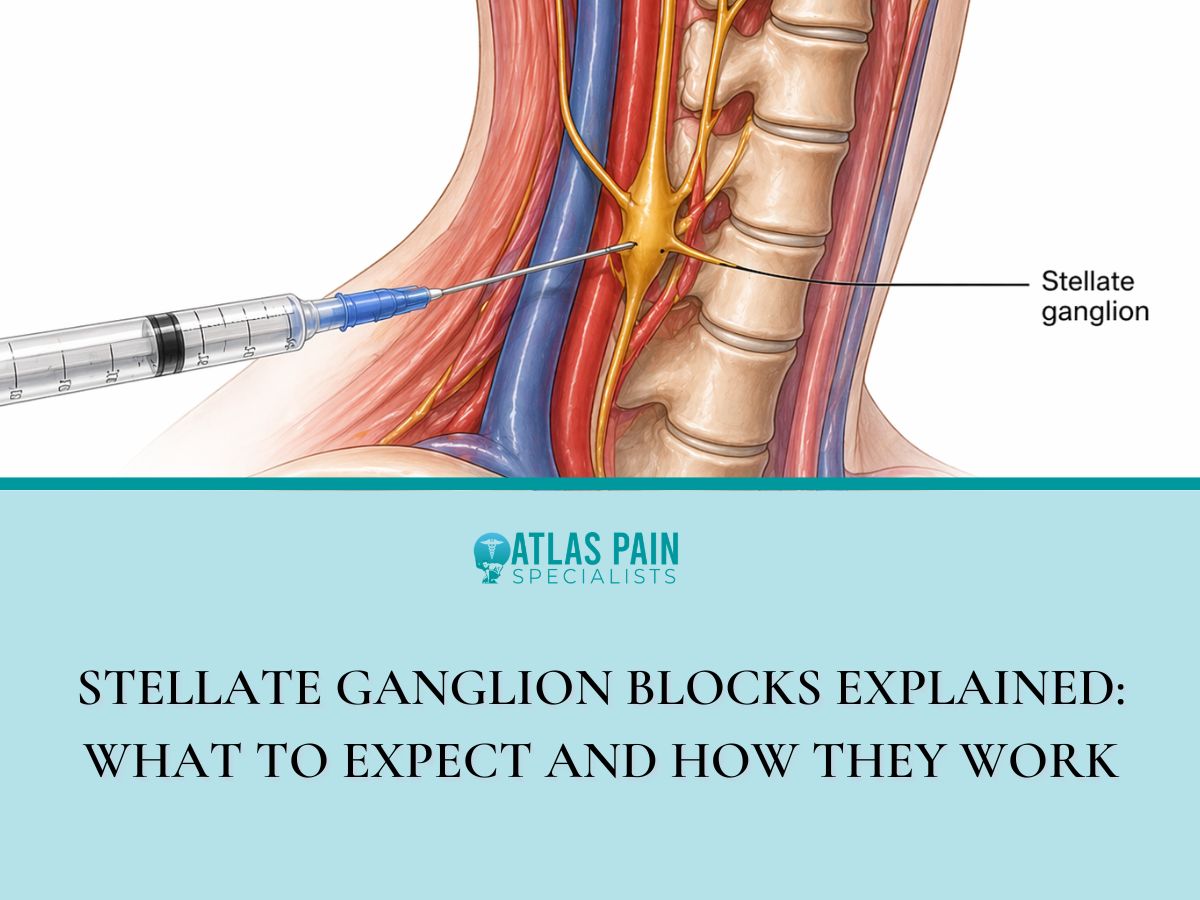
The stellate ganglion is a collection of nerve cell bodies located at the level of the lower neck, specifically between the C7 and T1 vertebrae. This structure measures roughly 1 centimeter in size and resembles a star, which gave it the name "stellate" from the Latin word for star.
- Location and Anatomy
The ganglion sits just in front of the longus colli muscle and behind the carotid artery and internal jugular vein. Its position near the esophagus and trachea explains why a block can temporarily cause hoarseness or a droopy eyelid.
- The Sympathetic Chain Connection
This nerve cluster belongs to the sympathetic nervous system, which controls involuntary functions like heart rate and blood vessel constriction. The stellate ganglion specifically sends signals to the head, neck, arms, and upper chest.
What the Stellate Ganglion Does
- It constricts blood vessels in the upper limb and face
- It controls sweating on the same side of the body
- It dilates the pupil and lifts the eyelid
- It helps regulate heart rate through nerve branches to the heart
Each of these functions serves a protective purpose during physical threat or injury. When the ganglion fires too often without a real threat, those same actions cause problems like cold hands, facial sweating, or a racing pulse.
How the Block Actually Works
The procedure deposits a small volume of local anesthetic, usually lidocaine or bupivacaine, directly around the stellate ganglion. This anesthetic temporarily stops the nerve from sending electrical signals along the sympathetic chain.
- The Mechanism of Nerve Blockade
Local anesthetic molecules enter the nerve cell membrane and bind to sodium channels. This binding prevents sodium from entering the cell, which blocks the action potential from traveling further.
Without a propagating action potential, the ganglion cannot relay pain signals or vasoconstrictor commands to the upper body. The result is a temporary chemical shutdown of that specific nerve cluster.
- What Resetting Means Physiologically
A successful block interrupts the feedback loop of chronic sympathetic overactivity. The nerve does not get damaged or destroyed, only silenced for several hours.
After the anesthetic wears off, the ganglion often resumes a lower baseline firing rate. This reset effect can last weeks or months in some patients.
- Immediate Physical Changes After Injection
Blood vessels in the blocked side dilate, which causes visible redness and measurable warmth in the hand and arm. Sweating stops on that same side of the face and upper limb.
The pupil constricts slightly and the upper eyelid droops, a combination called Horner syndrome. These signs confirm accurate anesthetic placement and predict a better clinical outcome.
Who Usually Gets This Injection
The stellate ganglion block has regulatory approval for several pain conditions but remains off-label for most psychiatric uses. A pain management physician or anesthesiologist typically determines candidacy based on symptom pattern and prior treatment failures.
- Complex Regional Pain Syndrome (CRPS)
CRPS patients experience burning pain, swelling, and skin color changes in one arm after a minor injury or surgery. The block can interrupt the sympathetically maintained pain that drives this condition.
A positive response to a diagnostic block predicts good outcomes from a series of therapeutic blocks. Many CRPS patients receive three injections spaced two weeks apart for optimal relief.
- Post-Traumatic Stress Disorder (PTSD)
Military veterans and civilian trauma survivors with PTSD have shown symptom reduction after stellate ganglion block. The proposed mechanism involves resetting an overactive amygdala response to non-threatening stimuli.
Clinical studies report decreased hypervigilance, fewer nightmares, and lower anxiety scores post-injection. The effect appears within one hour and can last several weeks.
- Long COVID and Post-Viral Syndromes
Patients with long COVID often present with inappropriate tachycardia, temperature dysregulation, and fatigue. These symptoms mirror sympathetic overdrive and respond to stellate ganglion blockade in small case series.
Early data suggests the block may reduce brain fog and improve sleep quality. Research continues to define which long COVID subgroups benefit most.
- Phantom Limb Pain and Herpes Zoster
Amputees who feel burning or cramping in a missing limb sometimes gain relief from this injection. The same procedure can reduce the shooting pain of post-herpetic neuralgia after shingles.
These conditions share a component of sympathetically maintained pain. The block offers an alternative when oral medications fail or cause intolerable side effects.
What Happens Right Before the Procedure
A pre-procedure evaluation includes a review of current medications and a brief neurological exam. The physician asks about any history of bleeding disorders or allergic reactions to local anesthetics.
- Medication Adjustments
Blood thinners such as warfarin, apixaban, or clopidogrel require a temporary hold before the injection. The physician provides specific stop dates based on each drug's half-life.
Non-steroidal anti-inflammatory drugs like ibuprofen or naproxen may also need a pause for three days. Aspirin at low doses for heart protection often continues with physician approval.
- Positioning and Monitoring
The patient lies flat on an examination table with the head turned slightly away from the injection side. A small roll or pillow supports the neck to expose the anterior cervical spine.
An intravenous line is placed for emergency access although serious complications remain rare. Standard monitors track heart rate, blood pressure, and oxygen saturation throughout the brief procedure.
- Imaging Guidance Setup
A high-frequency ultrasound probe sits on the side of the neck to visualize the carotid artery, thyroid, and nerve roots. The physician identifies the stellate ganglion at the C7 level near the longus colli muscle.
Fluoroscopy, a live X-ray technique, serves as an alternative when ultrasound cannot clearly show bony landmarks. Both methods confirm needle tip position before anesthetic injection.
Step by Step During the Injection
The skin over the lower neck receives a small wheal of lidocaine to numb the needle entry site. This superficial injection burns for several seconds then fades to complete numbness.
- Needle Placement
A three-inch, 25-gauge needle advances through the numbed skin toward the stellate ganglion. The physician watches the needle tip on the ultrasound screen or fluoroscope to avoid the carotid artery and vertebral vessels.
Gentle aspiration confirms the needle has not entered a blood vessel. A small amount of contrast dye may be injected under X-ray to verify spread around the ganglion.
- The Anesthetic Injection
5 to 10 milliliters of local anesthetic, usually lidocaine 1% or ropivacaine 0.2%, passes slowly through the needle. The patient feels deep pressure but not sharp pain during the injection.
The medication spreads along the fascial plane surrounding the sympathetic chain. A successful injection produces a visible change in tissue appearance on ultrasound.
- Sensations During the Injection
A warm flush travels down the arm on the injected side within 30 to 60 seconds. The hand may feel heavy or tingly as blood vessels dilate.
Some patients report a metallic taste in the mouth or a feeling of a lump in the throat. These sensations pass within a few minutes and do not indicate any problem.
- Duration of the Needle Procedure
The entire needle placement and injection process takes less than 10 minutes from start to finish. The patient remains awake and can report any unusual symptoms immediately.
Right After the Block What You Will Notice
The patient stays in a recovery area for 15 to 30 minutes after the injection. A nurse checks vital signs and monitors for any signs of local anesthetic toxicity or allergic reaction.
- Horner Syndrome Signs
The upper eyelid on the injected side droops slightly, a condition called ptosis. The pupil becomes smaller than the other side, which is miosis.
These two findings together confirm sympathetic blockade of the eye and face. The changes look concerning but cause no harm to vision or eye function.
- Voice and Throat Changes
The recurrent laryngeal nerve sits close to the stellate ganglion and may catch some anesthetic spread. This produces a hoarse or breathy voice that lasts 1 to 2 hours.
Some patients feel a lump in the throat or notice difficulty swallowing saliva. These symptoms resolve completely as the anesthetic wears off.
- Arm and Hand Findings
The injected side arm and hand turn pink or red from increased blood flow. The skin temperature rises by 1°C to 3°C compared to the other arm.
Sweating stops completely on the palm and forearm of the treated side. Patients often describe the arm as feeling warm, heavy, or slightly numb.
- Timeline for Resolution
Horner syndrome typically fades within 2 to 4 hours after the injection. The hoarse voice usually clears within 90 minutes.
The increased blood flow and warmth can persist for several hours to several days. This prolonged effect indicates a successful and durable nerve blockade.
Possible Side Effects and Risks
Most side effects from a stellate ganglion block are temporary and relate to the spread of local anesthetic to nearby structures. Serious complications occur in fewer than 1% of procedures when performed with imaging guidance.
- Common Temporary Side Effects
Hoarseness from recurrent laryngeal nerve block affects approximately 30% of patients. This resolves completely within 1 to 2 hours without any treatment.
Difficulty swallowing or a sensation of food sticking in the throat occurs less frequently. Patients should sip liquids slowly until normal swallowing returns.
Temporary Horner syndrome, including droopy eyelid and small pupil, happens in nearly every successful block. These signs reverse as the anesthetic wears off.
- Injection Site Issues
Bleeding under the skin at the needle entry point produces a small bruise that fades within 1 week. A tiny collection of blood called a hematoma may feel firm to the touch but resolves on its own.
Infection at the needle site presents as increasing redness, warmth, and tenderness after the first day. Oral antibiotics treat this rare complication effectively when caught early.
- Rare But Serious Risks
Seizure from accidental injection of local anesthetic into a blood vessel requires immediate treatment with intravenous lipid emulsion. Physicians prepare this rescue medication before every nerve block procedure.
Pneumothorax, or a punctured lung, occurs when the needle goes too deep and enters the pleural space. This complication causes chest pain and shortness of breath and requires chest tube placement.
Spinal cord injury or epidural spread of anesthetic is extraordinarily rare with ultrasound guidance. Permanent nerve damage has been reported but only in case reports spanning several decades.
Dorsal Root Ganglion Stimulation Procedure: How It Works
The stellate ganglion block offers a temporary reset for an overactive sympathetic nerve cluster in the neck. Patients with CRPS, PTSD, or long COVID may find significant relief from a single injection or a short series of three.
A related but distinct procedure targets a different nerve structure called the dorsal root ganglion. The dorsal root ganglion lies inside the spinal canal and controls sensory signals rather than sympathetic fight-or-flight responses.
While the stellate ganglion block numbs nerves outside the spine, dorsal root ganglion stimulation modulates pain signals at their spinal entry point. Both interrupt pain pathways in different ways, and patients who fail one may still respond to the other.
About Dr. Sean Ormond

Dr. Sean Ormond is dual board-certified in Anesthesiology and Interventional Pain Management. He completed his anesthesia residency at Case Western University in Cleveland, Ohio where he served as Chief Resident, followed by an interventional pain management fellowship at Rush University in Chicago, IL. Following fellowship, Dr. Ormond moved to Phoenix and has been practicing in the Valley for a few years before deciding to start his own practice.